Authors: Tom Latham
Link to PDF chapter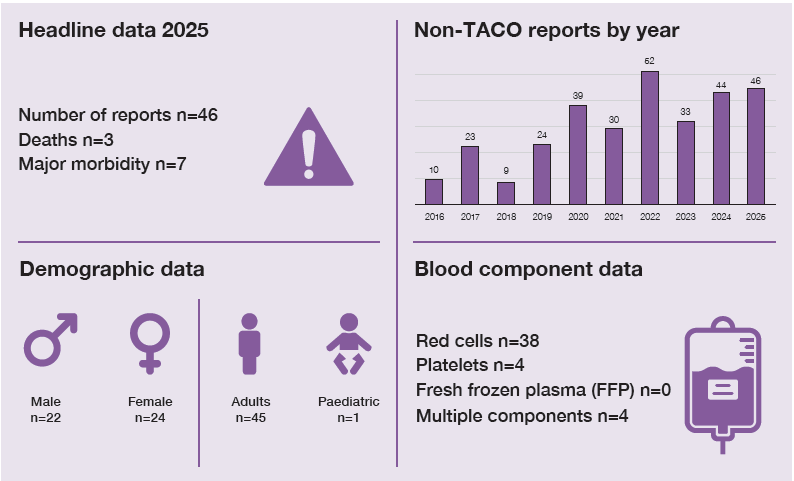
Key SHOT messages
Key findings
- Most cases were transfusion-associated dyspnoea (TAD), (n=41) and the remaining 5 cases were classified as transfusion-related acute lung injury (TRALI).
- There were no reported cases of antibody-mediated TRALI or TRALI type I.
- Fluid overload was considered likely to have contributed to approximately half of TAD cases but transfusion-associated circulatory overload (TACO) criteria were not met.
Gaps identified
- Missing information in submitted reports limits categorisation of analysed cases as TACO in accordance with the validated definition. Pre-existing conditions are not covered in the current definitions and may result in some cases with fluid overload being missed.
- Missed opportunities for learning from the pulmonary cases continue to be evident.
Good practice
- Increasing use of TACO pre-transfusion risk assessment and assessment tools.
- Evidence that most cases of suspected TRALI are reported to Blood Services.
Next steps
- Increased reporting of imaging, oxygenation changes, brain natriuretic peptide (BNP) measurements and previous clinical condition may reduce classification as TAD.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Non-TACO pulmonary complications definition
Cases where there is a respiratory deterioration within 24 hours of transfusion which does not
meet International Society of Blood Transfusion (ISBT) TACO criteria, and which is not explained by the recipient’s underlying condition.
For a more detailed definition see https://www.shotuk.org/reporting/incident/definitions/
Introduction
There were 66 cases submitted or transferred from other categories. Of these, 12 were withdrawn as
they were either of insufficient severity or due to the underlying condition, and 8 cases were transferred to TACO. This is detailed in the supplementary information.
Cases were classified using the International Revised Consensus (IRC) definitions of TRALI. Cases
satisfying both TRALI (Vlaar, et al., 2019) and TACO (Wiersum-Osselton, et al., 2019) criteria were
categorised as TRALI-TACO and cases satisfying neither as TAD. The TAD category is subclassified
into TAD-IC (cases which could not be classified because of incomplete information reported) and
TAD-C (cases where there was sufficient information to judge that the case did not meet either TACO
or TRALI criteria).
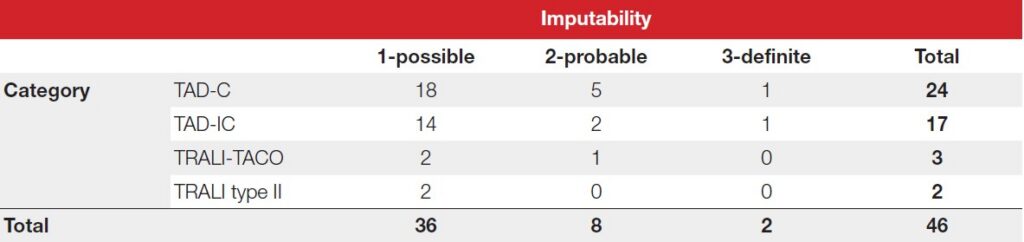
The final classification of cases with imputability is presented in Table 21b.1. Half of the cases (23/46)
were considered likely to have had fluid as a contributory or causative factor based on clinical judgement but did not meet TACO reporting criteria.
Table 21b.1: Final classification of non-TACO cases in 2025 (n=46)
Deaths related to transfusion n=3
There were 3 deaths related to transfusion, all categorised as TAD with low imputability and multiple
comorbidities.
Case 21b.1: TAD-C pulmonary oedema after transfusion not satisfying TACO or TRALI definitions (imputability 1 – possible)
A patient of advanced age with pulmonary fibrosis was admitted due to breathlessness; there was renal impairment, pneumonia and a haemoglobin of 69g/L. They deteriorated 40 minutes into a red cell transfusion with pulmonary oedema on imaging. There were no cardiovascular changes, and they worsened despite receiving a diuretic. They died from respiratory failure the following day after declining ventilation.
TRALI was recorded on the death certificate, but the case does not meet TRALI criteria because the pretransfusion respiratory state was considered as ‘deteriorating.’ The case has been retained as TAD-C rather than excluded as there did appear to be a discrete change in condition during the transfusion.
Major morbidity n=7
All cases of major morbidity were of low imputability, with 5 cases classified as TAD, 1 as type 2 TRALI
and 1 as TRALI-TACO.
TRALI and leucocyte antibody cases n=5
There were no cases associated with leucocyte antibodies and no cases of type 1 TRALI. Three cases
were categorised as TRALI-TACO and 2 as type 2 TRALI. Both type 2 TRALI cases were associated with massive haemorrhage, which is itself a cause of acute respiratory distress syndrome. Two cases
classified as TRALI or TRALI-TACO were investigated for antibodies and were negative.
Of the cases referred this year as TRALI (regardless of final classification), 9/12 were discussed with a
Blood Service, suggesting that the majority of suspected cases are being reported appropriately and
the continuing low number of cases is unlikely to be due to a fall in reporting. It may sometimes be
appropriate for Blood Services not to investigate cases where the TRALI categorisation is clear and
there are many donors, but it remains unclear where the appropriate dividing line is. It also remains an open question how well the IRC TRALI criteria predict the finding of leucocyte antibodies in donors.
Case 21b.2: TRALI type 2
A patient was admitted with a single stab wound, grade 2 liver injury, and large volume
haemoperitoneum. A laparotomy was performed and 15 units of red cells, 14 units of FFP, two
adult therapeutic doses of platelets and two units of cryoprecipitate were transfused. About 6
hours after transfusion, the patient became hypoxic with SaO2 65%, hyperexpanded lungs and
bronchospasm. There was no response to diuretic. Chest X-ray (CXR) showed bilateral infiltrates. The patient required 3 days of mechanical ventilation.
The case was discussed with the Blood Service, and a decision was made not to investigate the donors as this would be uninformative with the large number of donors involved. The case met TRALI type 2 criteria on clinical grounds. Assuming a prevalence of antibodies in parous female donors of 32% (Lucas, et al., 2012), and a 1% prevalence in male donors, there would be a 94% probability of finding a donor with cognate antibodies by chance, regardless of actual causation.
TAD cases – can we learn anything from these?
TAD-IC cases – missing information
The main reason for classifying cases as TAD-IC was the inability to apply TRALI criteria because of
missing imaging or oxygenation data. Of 17 TAD-IC cases, 10 had no post-transfusion imaging and
6 had no post-transfusion oxygen saturation reported. The remaining case was administered diuretic
treatment, but no response was reported. Despite missing clinical information 9/17 cases were thought likely to be due to fluid overload. Complete and accurate case information is essential to enable reviewers to make reasonable assessments and to support meaningful learning from cases submitted to SHOT. However, it is acknowledged that detailed laboratory or radiological investigations may not always be appropriate in some patients, for example in patients on end-of-life care.
TAD-C cases
Similarly, about half (11/24) of cases classified as TAD-C were thought likely to be due to fluid overload but with insufficient clinical details provided to meet the TACO definition. All of these were considered at high risk of fluid overload based on the patient’s medical history. While 5 cases satisfied 2 of the qualifying TACO criteria (3 criteria are required), pre-existing risk is not considered when classifying TACO.
Many of the remaining cases were of low imputability with other potential explanatory factors. It is
challenging to objectively decide whether to include such cases as TAD-C or withdraw them. There is
a low threshold for including cases as there is no way of proving that the transfusion did not contribute to deterioration. Objective evidence of progression of an alternative pathology such as pneumonia on X-ray and a history of steady deterioration rather than a sudden change associated with transfusion would favour withdrawal. Detailed narrative of the previous clinical state and the reaction are the most helpful features to report.
There are a residual number of cases which cannot be explained by fluid overload, acute lung injury
or the patient’s underlying condition. While these cases were all self-limiting and improved with other measures such as bronchodilator therapy, they are a reminder that there are other mechanisms of respiratory deterioration other than the development of pulmonary oedema.
Case 21b.3: Dyspnoea associated with hypocalcaemia during red cell exchange
A patient with sickle cell disorder developed tachycardia, hypoxia and breathlessness during a
regular planned exchange transfusion. There were classical features of hypocalcaemia such as
tetany and paraesthesia. There was a clear CXR and normal post-transfusion BNP. They improved quickly after administration of a fluid bolus and calcium and were discharged the following morning.
Concordance with previous recommendations
The TACO pre‑transfusion risk assessment supports identification of patients vulnerable to pulmonary complications beyond TACO, recognising the role of fluid overload and inflammation. Where data was provided, the TACO pre-transfusion risk assessment was completed in 45/63 (71.4%) of submitted reports (including cases eventually withdrawn) which is increased from 2024 (31/47 [66.0%]) and 2023 (18/52 [34.6%]). Use of structured TACO investigation increased (29/61 [47.5%] vs 17/43 [39.5%] in 2024).
Conclusion
The pattern and number of non-TACO respiratory complications is similar to previous years, with a
majority of cases classified as TAD with low imputability in multiply comorbid patients. Fluid overload is suspected to contribute to a substantial proportion of cases even if TACO criteria are not met. Increased reporting of imaging, oxygenation changes, BNP measurements and previous clinical condition may help reduce the number of cases classified as TAD but may not always be practical.
Management of the risk of fluid overload and carefully considering the risk/benefit balance of transfusion remain the mainstay of prevention.