Author: Anne Kelly
Link to PDF chapter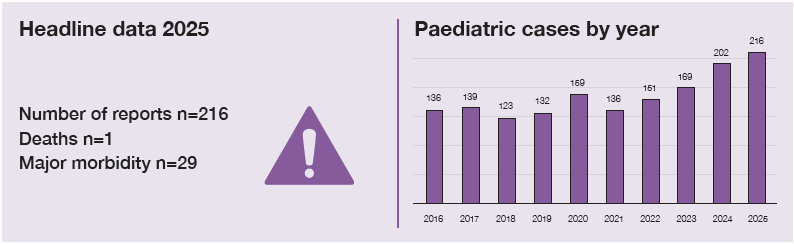
Key SHOT messages
Key findings
- The number of paediatric cases has risen over the last 5 years.
- For complex cases of haemolytic disease of the fetus and newborn (HDFN) it is vital that the transfusion requirements are discussed with the hospital laboratory prior to birth.
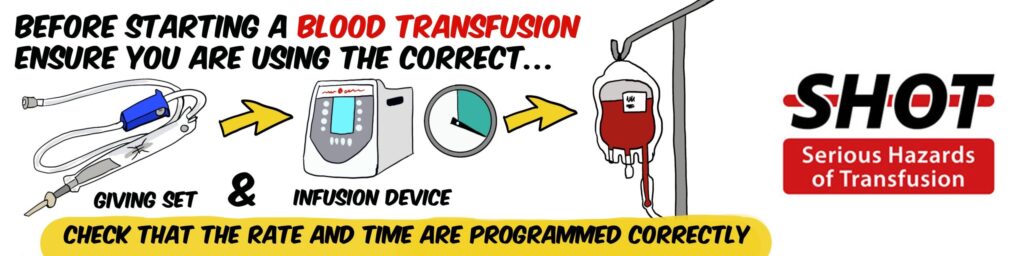
- Using incorrect giving sets can result in significant error in volume transfused.
Gaps identified
- Failure to use concessionary release continues to be an area of concern for paediatrics.
- A lack of communication of transfusion history between Trust/Health Boards and between clinical and laboratory teams.
- Insufficient education around the use of the correct giving set for transfusion.
Good practice
- Reporting allows areas of concern to be highlighted and targeted for transfusion education.
Next steps
- A new resource, the SHOT Concessionary Release Toolkit, is being developed to aid laboratories in decision-making around the provision of components in emergency situations. This will be available later in 2026.
- Review training programmes to include education around giving sets and report any issues with giving sets to SHOT and the Medicines and Healthcare products Regulatory Agency (MHRA) (via the Yellow Card scheme).
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Paediatric cases definition
Paediatric cases comprise all reports for patients under 18 years of age, including all paediatric cases from the other chapters in this report. Paediatric reports have been subdivided by recipient age group: neonates ≤28 days; infants >28 days and <1 year; children ≥1 year to <16 years and young people aged 16 to <18 years.
Introduction
The total number of reports is similar to last year; 216 in 2025 versus 202 in 2024, but with a continual rise in cases since 2021 (Figure 26.1). Paediatric cases account for 216/2381 (9.1%) of total reports if near miss (NM) and right blood right patient (RBRP) are excluded and 340/4046 (8.4%) if included.
Figure 26.1: Trends in paediatric SHOT reports 2016-2025
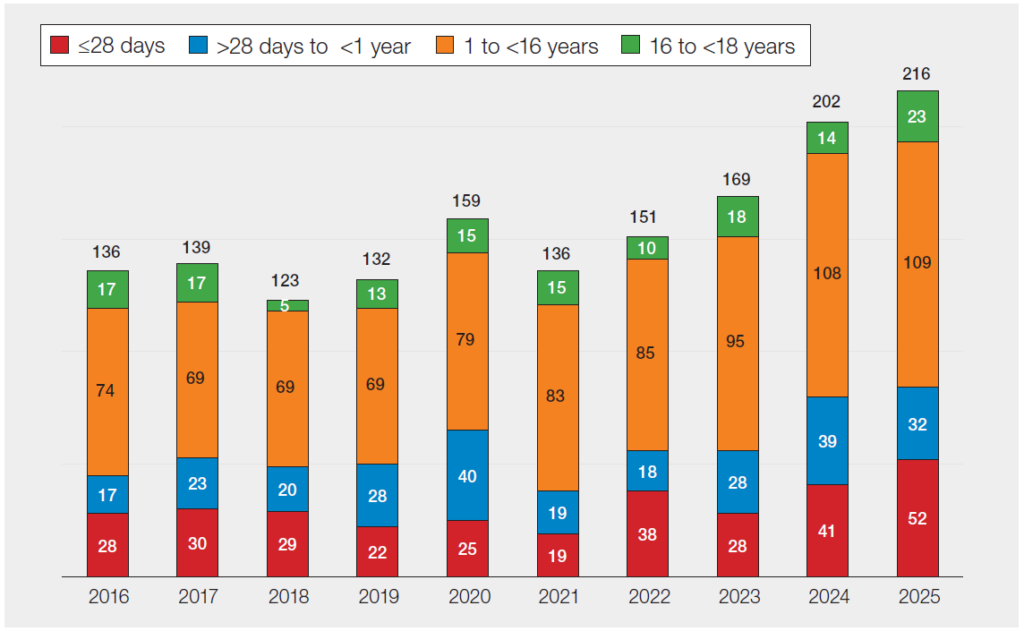
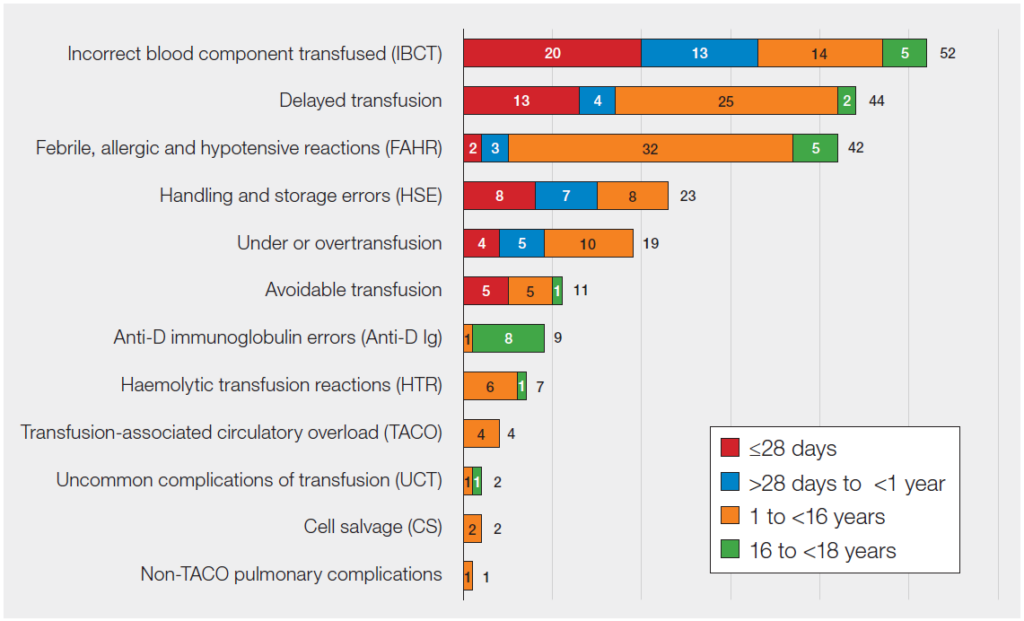
Figure 26.2: Summary of paediatric cases by category and age in 2025 (n=216)
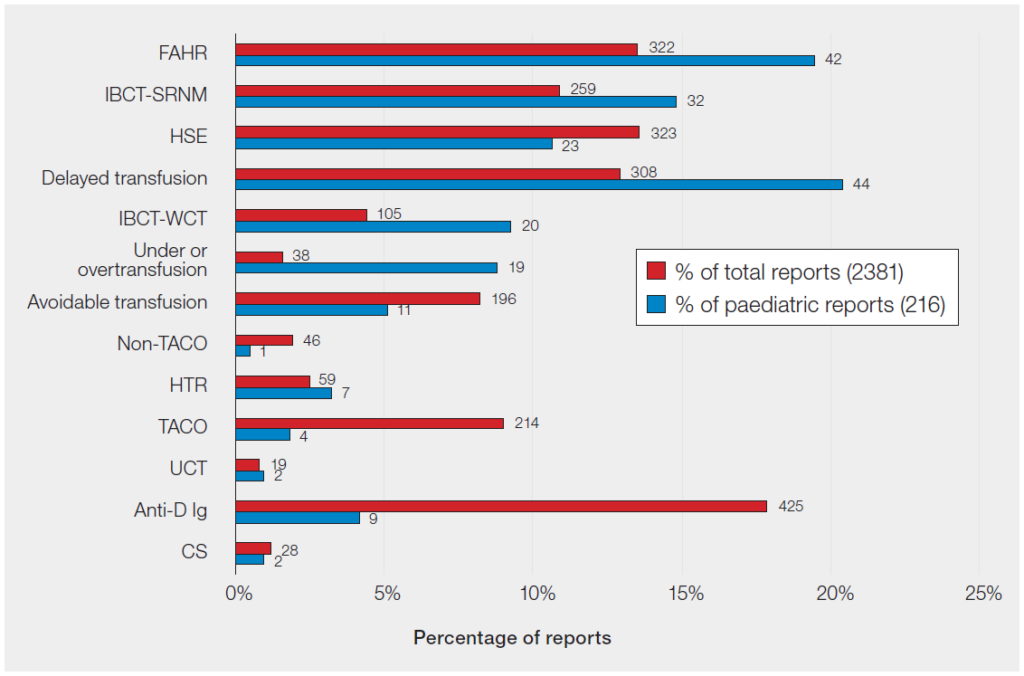
In 2025 the same patterns were seen as last year in that paediatric reports are over-represented in FAHR, IBCT, delayed and under/overtransfusion, UCT and in HTR (Figure 26.3).
Figure 26.3: Percentages of paediatric and total reports in each category in 2025 (n=216)
Deaths related to transfusion n=1
There was 1 death possibly related to delayed transfusion (Case 26.1). This was a case of failure to issue components under concessionary release in an emergency situation. To help address this issue, a SHOT concessionary release toolkit is being developed (see ‘Recommended resources’).
Case 26.1: Transfusion delay and death in a neonate (imputability 1 – possible)
There was a 23-minute delay in provision of red cells to a neonate who was born in poor condition due to placental abruption. Urgent neonatal/infant red cells were requested following birth; however, collection of adult O D-negative units present on site in the maternity refrigerator was not considered. A further delay occurred when a biomedical scientist (BMS) was unable to access the theatre to deliver the unit urgently.
Learning point
- If clinical urgency dictates that a neonate or infant cannot wait for neonatal/infant specification components, concessionary release and use of adult-specification components should be considered by clinical and laboratory staff.
Major morbidity n=29
There were 29 cases of major morbidity. The most common category was FAHR with 21 cases, followed by 4 cases of TACO. Of note, all TACO cases in children were associated with major morbidity. The remaining cases were 2 delayed transfusions and 2 HTR.
Error related reports n=160
Paediatric error reports have continued to increase year-on-year. Clinical errors, 99/160 (61.9%), remain more common that laboratory errors, 61/160 (38.1%), and the proportion of clinical errors has increased further from 54.3% in 2024.
Incorrect blood component transfused (IBCT) n=52
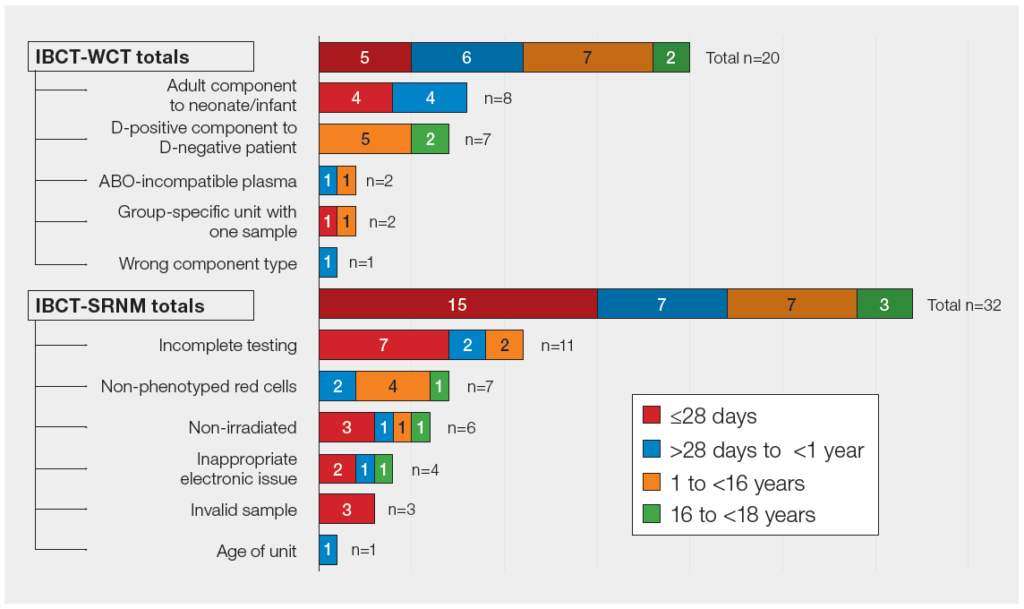
Laboratory errors predominate in this category for both IBCT-WCT and IBCT-SRNM. These reports are particularly prominent in neonates and infants, reflecting the complexity of laboratory testing and component specifications in this age group (Figure 26.4).
Figure 26.4: Breakdown of incorrect blood component transfused reports in 2025 (n=52)
Incorrect blood component transfused – wrong component transfused (IBCT-WCT)
n=20
IBCT-WCT clinical errors n= 9
On 5 occasions adult O D-negative emergency red cells were given to a neonate in error (see Case 26.2). There were 2 cases of O D-positive components being given to O D-negative patients, 1 case where the second group and screen sample was invalid as it had been taken at the same time as the first sample, and 1 incorrect component type transfused.
Case 26.2: Use of emergency O D-negative adult units for a neonate with maternal antibodies
A neonate with known HDFN secondary to maternal antibodies (anti-e, anti-C, anti-Kpa) had a strongly positive (4+) direct antiglobulin test (DAT) at birth. Antigen-negative units had been ordered for the mother and were available in the hospital. Shortly after birth the laboratory was alerted that a unit of adult emergency group O D-negative red cells had been removed from the satellite refrigerator and transfused to the baby. This was authorised by the neonatal consultant due to the poor clinical condition of the neonate at birth. The transfusion laboratory staff communicated to the clinical team that the emergency red cells were not the best choice for this child going forward, however later that day a further O D-negative adult unit was transfused. It transpired that the birth plan specified the use of O D-negative for the neonate until an exchange unit was available. The baby received further treatment and survived.
This case highlights the need to strengthen clinical knowledge and communication between clinical and laboratory teams, around the appropriate choice of component in the context of maternal antibodies. In an emergency where red cells are required immediately, transfusion of O D-negative units would be appropriate. However, in this case there were antigen-negative adult specification red cells available in the laboratory which would have been a better subsequent choice for this child.
Learning points
- The transfusion requirements of complex HDFN cases should be discussed with the hospital transfusion laboratory and consultant haematologist prior to delivery.
- In cases where there is complex maternal serology, discussion with Blood Services can help to ensure appropriate provision of suitable blood for both mother and infant.
IBCT-WCT laboratory errors n=11
Five of these reports involved D-positive components being transfused to D-negative or undetermined D-status recipients. Three resulted in neonatal/infant specification components not being provided when there was time to do so. The final 3 cases were grouping errors, 1 of which highlights the importance of communication when patients are transferred between hospitals (Case 26.3).
Case 26.3: ABO-incompatible fresh frozen plasma (FFP) administered to an infant wrongly assigned as group O
A group B D-positive infant was transferred to a different hospital. At the receiving hospital, the infant appeared to be group O D-negative on testing and therefore group O FFP was issued. The infant had been transfused with a large amount of O D-negative red cells. Neither the ABO/D group of the infant nor the transfusion history had been communicated to the teams at the receiving hospital.
Incorrect blood component transfused – specific requirements not met (IBCT-SRNM)
n=32
The majority of IBCT-SRNM reports were laboratory errors, 24/32 (75.0%). There were 8 clinical reports all of which highlighted issues with communication. Cases 26.4 and 26.5 reflect the importance of communication of transfusion history and key clinical details which impact upon specific requirements. In 4 reports the requirement for irradiated components was not communicated, involving intrauterine transfusion (IUT), severe combined immunodeficiency (SCID), Di George and fludarabine treatment.
Case 26.4: Failure to provide an antigen-negative component for an infant with maternal anti-M
An infant (<4 months of age) whose mother had historical allogeneic anti-M received an M-unselected component in error. The unit was subsequently found to be M-positive. The infant’s DAT was negative, and no harm occurred.
Case 26.5: Inappropriate electronic issue for a child with sickle cell anaemia
A teenager was transfused with one unit of red cells issued via electronic issue rather than serological crossmatch. The transfusion laboratory was not informed that the patient had been transfused elsewhere and red cell antibodies had been detected. A sample had been sent away to a reference laboratory by the previous hospital for antibody identification and the results were available on a national antibody database. Even though this report was accessed, the patient’s record on the laboratory information management system (LIMS) was not updated. There was no adverse clinical effect.
Learning points
- Compatibility testing for infants <4 months of age must take into account maternal antibody status.
- Transfusion history for all patients, and maternal antibody status for patients <4 months of age, must be communicated between laboratories when patients are transferred between hospitals.
- A suggested communication form for neonates/infants is appended to the paediatric transfusion guideline (New, et al., 2016).
Avoidable transfusions n=11
In 5 cases of avoidable transfusion the error was due to acting upon inaccurate or historical results. There were also 4 cases of avoidable use of emergency O D-negative. In another case, flawed decision-making meant that a teenager had a platelet transfusion when the count was adequate for the planned procedures. In the final case a teenager continued to receive plasma and cryoprecipitate even though the major haemorrhage protocol had been stood down.
Delayed transfusions n=44
Transfusion delays were again prominent and occurred at all stages of the transfusion process. There was 1 death which is discussed in Case 26.1. A quarter of cases occurred due to lack of component availability (11/44), which included a delay in provision of red cells for an exchange transfusion in a neonate (Case 26.6).
Case 26.6: Delay in provision of red cells for neonatal exchange transfusion
A neonate who required an urgent red cell exchange transfusion for hyperbilirubinaemia had a 4-hour delay in the provision of red cells. The initial request occurred out-of-hours and the BMS was unclear about what component specification to order from the Blood Service. A component was ordered by the day staff with the support of the transfusion practitioner.
Learning points
- Neonatal red cell exchange transfusions are now rarely performed and are an area of vulnerability, clear protocols for the practicalities and process of exchange transfusion are therefore important.
- Blood Services provide specialist components for neonatal exchange transfusion and can be contacted for advice if required.
Communication problems were also prominent in reports of delay in transfusion (10/44). Choice of component will depend upon both ideal components required, current stock on site and clinical urgency and therefore a two-way conversation between clinical and laboratory teams is vital.
Case 26.7: Over 2-hour delay in provision of red cells for a severely anaemic neonate
A neonate was born with a haemoglobin (Hb) of 34g/L due to fetomaternal haemorrhage. The clinical team had some knowledge of neonatal components and asked for ‘Cytomegalovirus (CMV)-negative components (leucodepleted)’. The case was discussed with the haematology consultant on call, but the urgency and status of the baby was not communicated, resulting in a 2-hour delay whilst awaiting a neonatal/infant specification component from the Blood Service. The adult-specification O D-negative units which were available to use in an emergency were not given.
Learning points
- Clear communication about clinical urgency is essential when discussing complex cases with specialists regarding provision of blood components.
- If neonatal/infant specification components are not rapidly available and clinical urgency dictates, then concessionary release of adult-specification components is indicated.
Under and overtransfusion n=19
Transfusion dose calculation errors and pump programming errors continue to predominate as causes for under and overtransfusion particularly in neonates and infants.
Undertransfusion n=8
There were 8 cases of undertransfusion reported. In 4 cases these were pump programming errors resulting in the wrong rate, 1 was a lack knowledge of the appropriate dose of granulocytes for a child
and 2 were related to exchange transfusion in children with sickle cell anaemia.
The final case involved the use of the correct giving set for administration. This has been identified as an area of concern and was discussed both in the 2024 Annual SHOT Report and recent MHRA, Maternal & Newborn Safety Investigations and British Association of Perinatal Medicine safety alerts (Narayan, et al., 2025; MNSI, 2025; BAPM, 2025).
Case 26.8: An infant received an undertransfusion due to use of an adult-sized giving set
An infant received around 20mL less red cells than prescribed due to the use of an adult-sized blood giving set (via a volumetric pump) which has a larger priming volume than when given with a paediatric giving set. Pre-transfusion Hb was 68g/L and post-transfusion Hb was 79g/L.
Learning points
- It is vital that the correct type of paediatric blood giving set is used for infants and neonates to ensure the correct blood volume is administered.
- Use of an adult giving set for a child can result in undertransfusion due to a different priming volume.
- Use of a fluid giving set for blood components can result in an undertransfusion due to cells being trapped by the smaller filter (see Figure 26.5 and SHOT Bite 35).
Figure 26.5: Blood administration giving sets

Overtransfusion n=11
The majority of errors (7/11) were prescribing (including calculation) errors. The remaining cases were 3 pump programming errors (see Case 14.2) and 1 where staff acted on a mis-heard result (heard 116g/L when the Hb was actually 160g/L) during a stressful resuscitation situation.
Case 26.9: An infant was prescribed two adult units of red cells
A small transfusion-dependent infant was prescribed two adult units of red cells. The nursing team realised the error immediately prior to hanging the second unit of red cells. However, the child had already received 38mL/kg of red cells (maximum dose is 20mL/kg). No significant morbidity resulted from this error.
Learning points
- Prescribing for paediatric patients should be in mL (up to the equivalent of one adult therapeutic dose).
- The volume of red cells required for an infant or child can be calculated based on the current Hb and the desired rise, which is generally not more than 20g/L above the threshold. The formula will be simplified in the new version of the paediatric guideline due to be published later in 2026.
Cell salvage n=2
There were 2 reports related to cell salvage, 1 due to equipment malfunction and the other was haematuria in a patient following reinfusion of both salvaged and allogeneic red cells. It was unclear whether this was haemolysis or due to a urinary catheter.
Handling and storage errors (HSE) n=23
The majority of errors were clinical (20/23) with only 3 laboratory errors. The clinical errors included 9 due to pump programming errors, and 4 giving set errors. In 2 cases this related to broken or malfunctioning giving sets. The other cases were rapid infusion of platelets due to a clamp accidentally left open and the final case was administration of a platelet transfusion to a neonate via a pump but without a correct giving set.
Anti-D immunoglobulin (Ig) n=9
There were 9 cases of maternity anti-D Ig errors in older teenagers. Seven were omission or late administration and 2 were unnecessary administration.
Transfusion-related reactions n=56
Febrile, allergic and hypotensive reactions (FAHR) n=42
FAHR reports continue to be prominent in paediatrics with around 50% of reports being due to platelet transfusions (Figure 26.6). The majority of reports were in children >1 year of age (37/42). The difference between adult and paediatric FAHR cases is illustrated in in Figure 26.7a, showing the high prevalence of reactions to platelets in children.
Figure 26.6: Summary of paediatric FAHR reports by component 2016-2025
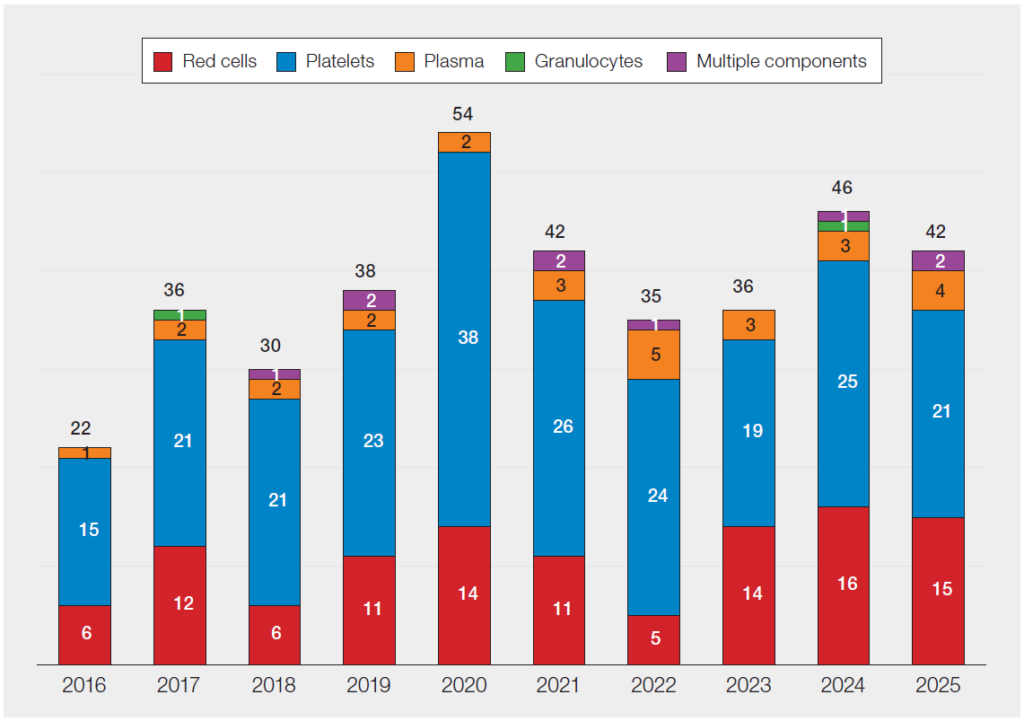
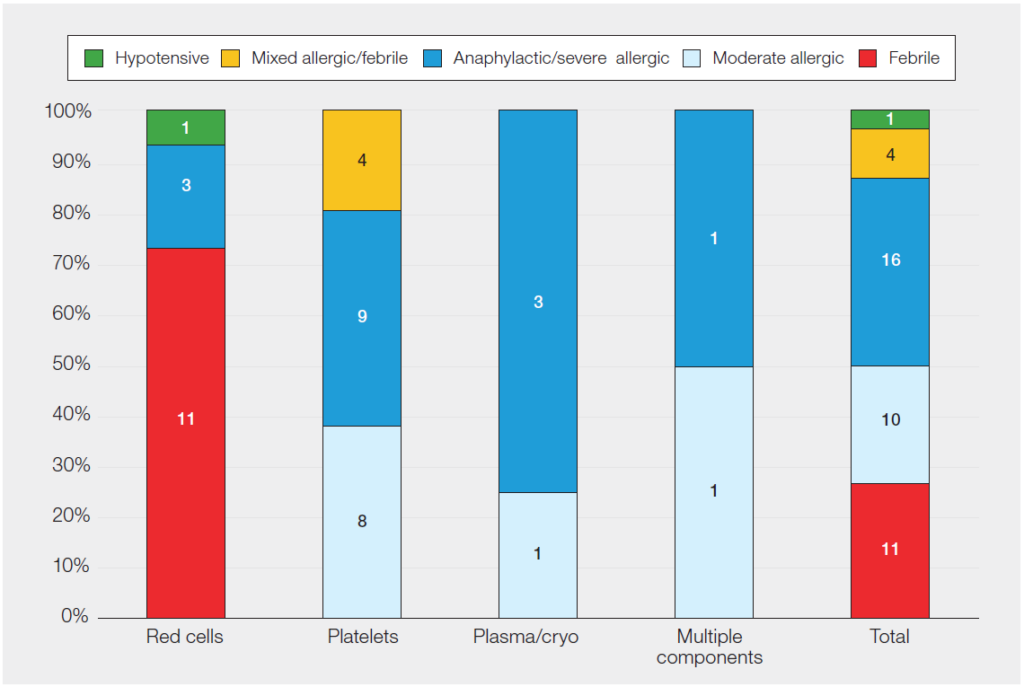
Figure 26.7: Paediatric FAHR reports in 2025 (n=42)
a: Comparison of proportions of adult and paediatric reports by component types
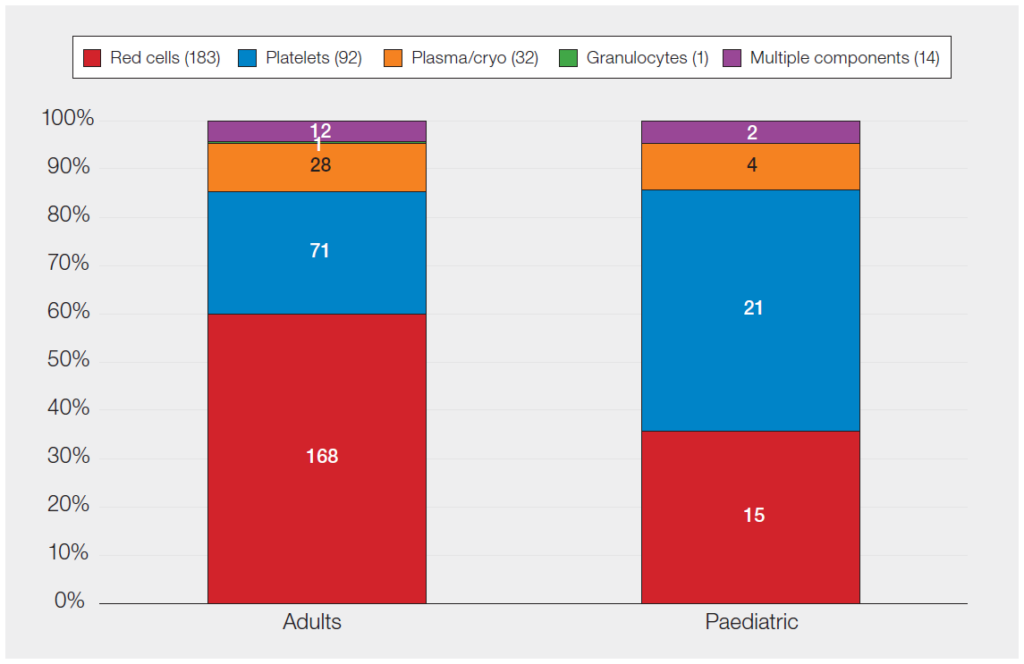
b: Percentages of reaction types in paediatric FAHR related to different component types
Haemolytic transfusion reactions (HTR) n=7
There were 7 haemolytic transfusion reactions in 2025. All occurred in children >1 year of age and 5/7 were in patients with sickle cell disorder, 1 patient had thalassaemia and the other was a complex medical patient having surgery.
Of the HTR cases, 5 were delayed reactions and of these 4 had developed a new antibody (anti-E, anti-Fya, anti-Jka and one patient developed anti-E, anti-M and anti-Lea). There were 2 cases of hyperhaemolysis, both involved patients with sickle cell disorder and were associated with major morbidity.
Pulmonary complications of transfusion in neonates and children n=5
Transfusion-associated circulatory overload (TACO) n=4
There were 4 TACO cases reported to SHOT in 2025. All were in the 1-15 years age group and all were
associated with major morbidity. All had at least 1 known adult TACO-related risk factor.
Case 26.10: TACO in a young child following a platelet transfusion
A young child with neuroblastoma who had previously received chemotherapy developed increasing shortness of breath 1-2 hours after a platelet transfusion. The child had also received intravenous fluids and exhibited respiratory symptoms. Pre-transfusion imaging showed some pulmonary congestion which worsened in post-transfusion imaging. The child responded to diuretics and supportive care in the paediatric intensive care unit.
Learning point
- TACO cases are not as commonly reported in paediatrics as in adults, but when reported, they are frequently associated with major morbidity.
Non-TACO pulmonary complications n=1
A young child had a drop in oxygen saturation following a red cell transfusion but also had concurrent
sepsis. There was no evidence of fluid overload.
There were no paediatric TRALI cases in 2025.
Transfusion transmitted infections (TTI) n=0
There were no paediatric cases of TTI in 2025.
Uncommon complications of transfusion (UCT) n=2
There were 2 UCT reports this year. The first was an older child who had reported non-specific leg pains and pins and needles 24 hours after red cell transfusion, and this had occurred on a number of occasions. The second was a teenager with sickle cell disorder who developed citrate toxicity during a red cell exchange transfusion.
Paediatric error reports with no harm n=124
Table 26.1: Paediatric error reports with no harm in 2025 (n=124)
| ≤ 28 days | 28 days – <1 year | 1 – <16 years | 16 – <18 years | Total | |
|---|---|---|---|---|---|
| RBRP | 9 | 5 | 14 | 3 | 31 |
| NM | 13 | 5 | 10 | 4 | 32 |
| NM-WBIT | 47 | 2 | 6 | 6 | 61 |
| Total | 69 | 12 | 30 | 13 | 124 |
Conclusion
The paediatric cases reported to SHOT continue to highlight the differences between adult and paediatric transfusion in both errors and reactions. Complexity of the transfusion process particularly in neonates in terms of giving sets, use of pumps, and rarely performed procedures such as exchange transfusion add to the vulnerability of this patient group.
Communication between different hospital transfusion laboratories when patients are transferred, and between laboratory and clinical teams is vital at all stages of a child’s life. In antenatal cases multidisciplinary discussions pre-birth will facilitate planning of transfusion requirements and appropriate availability of blood components for the neonate. For transfusion of young infants, maternal transfusion history allows safe selection of components meeting specific requirements. For all children, knowledge of transfusion history will help support safe transfer of patients and their care between sites. Effective communication of the degree of clinical urgency to laboratory teams will facilitate concessionary release where appropriate and will ensure that any specific requirements for a child are not missed.
Recommended resources
SHOT Concessionary Release Toolkit
SHOT Bite No.04: Paediatrics (neonates, infants and children)