Additional data tables and analysis not included in the main 2025 Annual SHOT Report.
Involvement of information technology n= 105
Figure 9.2: Involvement of information technology in anti-D Ig errors (n=74)
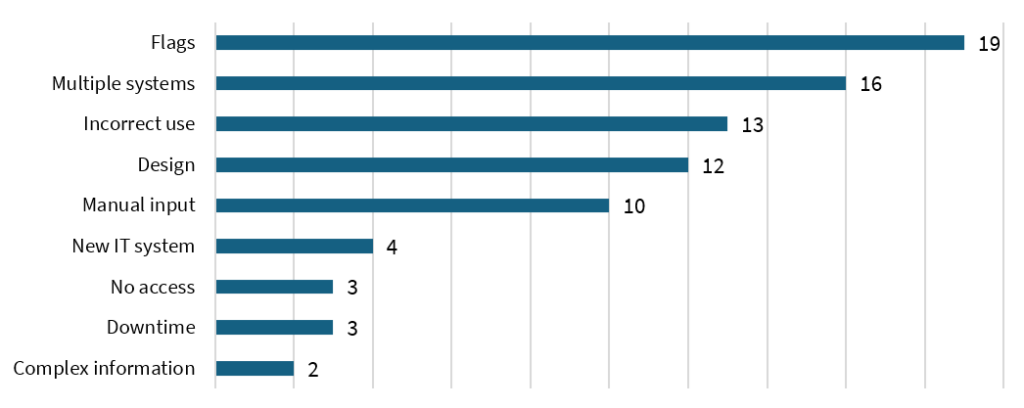
A further analysis of the impact of IT identified common gaps related to flags that influence decision-making, 19/74 either flags not present, present but not actioned, or appropriate flags not available. Another common contributory factor noted was a requirement to use multiple IT systems for result checking; 16/74 due to lack of interoperability/interfacing between IT systems from laboratory (reference and local), middleware and clinical settings. Incorrect use of the IT system accounted for 13/74 cases, mainly failure to review results or incorrect information (other than the D-status) entered. Additionally, there were 10 cases where the incorrect maternal or neonatal D-status was manually entered into the maternity IT system. SHOT has highlighted that manually inputting data poses a risk for patient safety, as discussed in the Problem Statement issued in August 2024 (see ‘Recommended resources’).
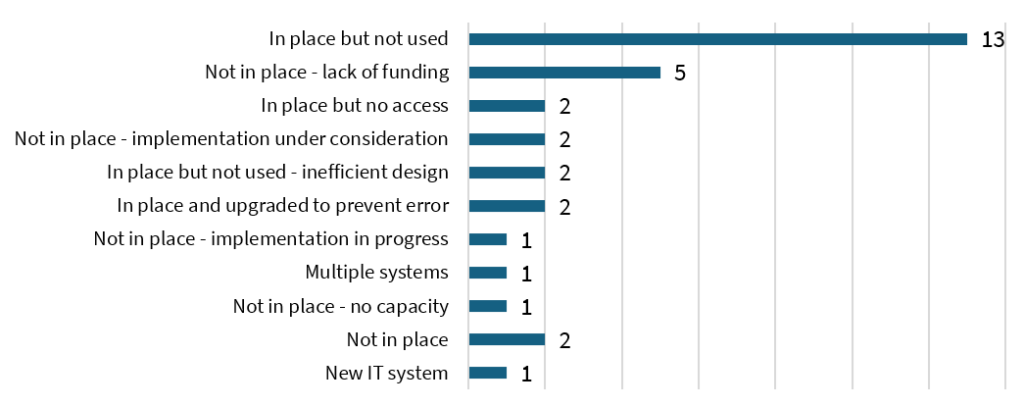
Figure 9.3: Anti-D Ig error cases where IT system could have prevented the error (n=31)
Non-invasive prenatal screening for RHD (cffDNA) n=76
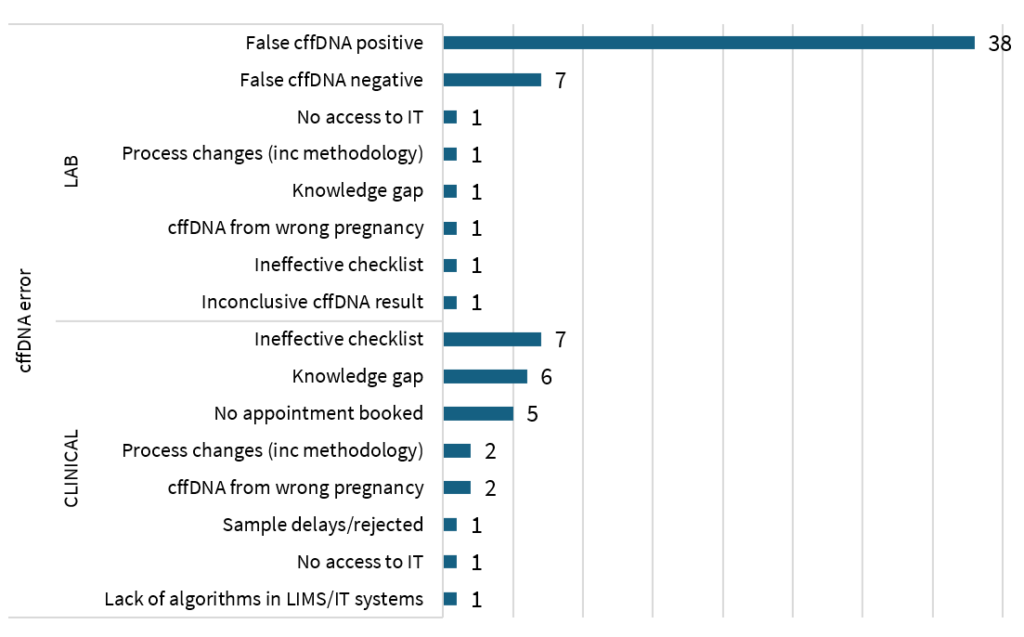
Figure 9.4: Causes of errors related to cffDNA screening reported by laboratory and clinical settings in 2025 (n=76)
Antenatal and postnatal care in non-maternity/gynaecology setting n= 8
Although only 8 cases were reported from outside obstetrics and gynaecology (OB/GYN) settings, further cases involved patients temporarily transferred out of these speciality areas. Where care in early pregnancy occurs outside of OB/GYN lack of familiarity with anti-D Ig requirements contributes to error. This is further hampered by current inconsistencies in national guidance of the anti-D Ig requirement for a PSE in the first trimester.
For those cared for outside OB/GYN settings, either in later pregnancy or postpartum, knowledge gaps and emergency care taking priority were cited as common contributory factors. Communication and handover have been identified as opportunities for improvement. Challenges include a lack of interfacing between EPR’s and omitting a verbal handover.
Case 9.3: Late administration of anti-D Ig due to emergency care and communication gaps
A woman was transferred from an external hospital to an ICU, due to sepsis, following the birth of still born twins. The external hospital was unable to obtain cord bloods and the cffDNA prediction was not handed over to the ICU. The ICU were not informed that the woman required anti-D Ig.
The omission was later detected by ward staff and anti-D Ig was administered outside of the 72-hour window. Following this case the ICU have added a question to their structured handover, asking if anti-D Ig is required or has been given. Learning from the case included an action that the laboratory should be notified of patients being transferred into the hospital, so that their records can be reviewed on Sp-ICE.
Failure to identify requirement for anti-D Ig (decision to omit) n=27
In 27/261 cases of the omitted or late administration, there was an inappropriate clinical decision to omit administration of anti‑D Ig; 22 were related to PSE, 4 to RAADP, and 1 to birth. The case of the omitted dose at birth was due to a misinterpretation of a negative direct antiglobulin test (DAT) in a cord sample by the clinician. The 4 omitted RAADP cases were due to assumptions that a dose given to cover a PSE would also cover RAADP. This highlights a knowledge gap in the appropriate management of pregnancy as per national guidance i.e., RAADP should be given despite the number of PSE and doses administered.
The decisions made to omit anti‑D Ig following PSE were multifactorial; assumptions were made that no additional doses were required as the woman or birthing person had a RAADP appointment scheduled soon or a dose of anti-D Ig that had been given recently for a different PSE would cover both (as shown in case X.2). There were also occasions where the clinicians did not consider small bleeds as PSE and consequently anti-D Ig was not requested. In 2 cases, the PSE was not managed appropriately due to complexities of the labour process; in one case, the clinician thought the woman was in labour, and when it was recognised that they were not, anti‑D Ig was not considered before discharge; and in another case, the dose given in labour was assumed to be sufficient to cover also the PSE.
Case 9.4: Unavailability of O D-negative emergency red cells units and knowledge gap leads to inappropriate management of a miscarriage
A patient became unstable during a surgical management of miscarriage with a sudden blood loss of 1.5L, a significant drop of blood pressure and increased heart rate. Due to the clinical presentation the medical team made the decision to transfuse the emergency group O D-positive units available in the satellite fridge. Emergency O D-negative units were not available as part of the local stock management following the activation of the national amber alert. Following the procedure the patient received 500iu anti-D Ig, but no sample was taken to estimate the volume or the requirement for additional anti-D Ig doses. The medical team assumed that the dose given for the miscarriage would be sufficient to cover the transfusion of D-positive red cells.