Authors: Heather Clarke, Nicola Swarbrick and Victoria Tuckley
Link to PDF chapter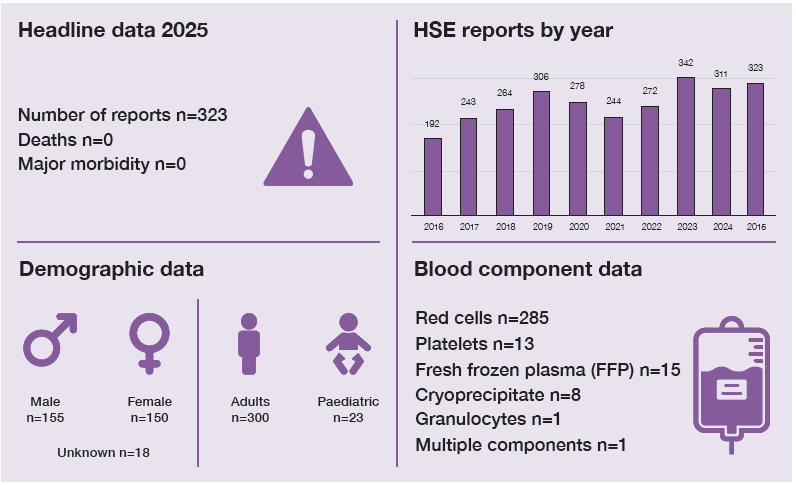
Key SHOT messages
Key findings
- Most HSE reports were due to clinical errors, over half being technical administration errors (including pumps and giving sets).
- Laboratory inappropriate return to stock errors doubled in 2025.
- Many reports involved excessive transfusion times.
Gaps identified
- Inadequate communication including handover between shifts/teams/individuals.
- Insufficient training, knowledge and competency assessments led to HSE errors.
Good practice
- Substantial decrease in laboratory refrigerator/equipment failure errors.
- Near miss errors once again showed that cold chain errors and expired units were identified in the pre-administration stage.
Next steps
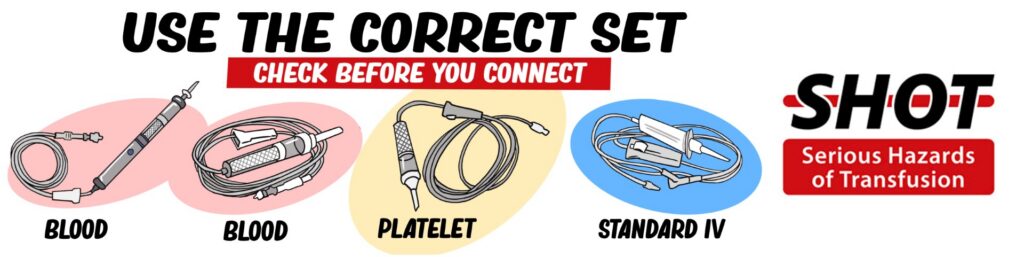
- Ensure correct use of blood giving sets in line with Medicines and Healthcare products Regulatory Agency (MHRA) guidance, include pumps and giving sets in training, and communicate transfusion end times during handover to avoid delays.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
HSE definition
Transfusion of the correct blood component to the intended patient, where handling or storage
errors may have rendered the component less safe for transfusion.
For a more detailed definition see SHOT Definitions
Introduction
HSE errors accounted for 323/4046 (8.0%) errors in 2025 compared with 311/3998 (7.8%) in 2024.
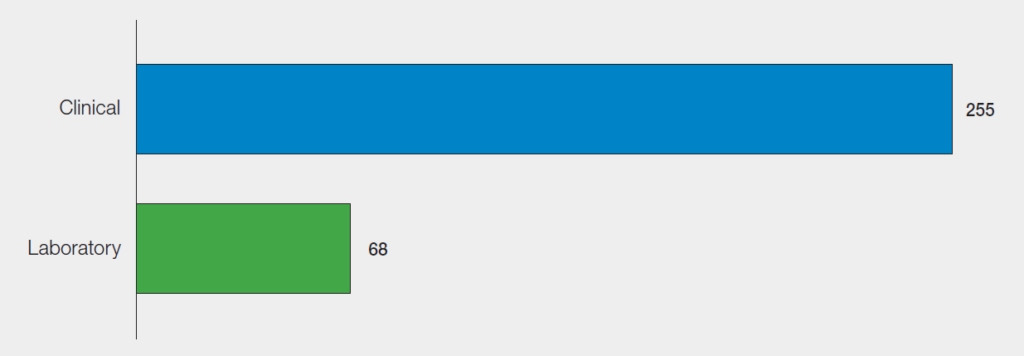
There were clinical errors in 255/323 (78.9%) reports, and laboratory errors in 68/323 (21.1%). The
variation between clinical and laboratory errors is illustrated in Figure 11.1.
Figure 11.1: Breakdown of 2025 handling and storage error (HSE) reports (n=323)
Deaths or major morbidity related to transfusion n=0
There were no deaths or major morbidity cases that were related to errors associated with HSE in 2025.
Clinical errors n=255
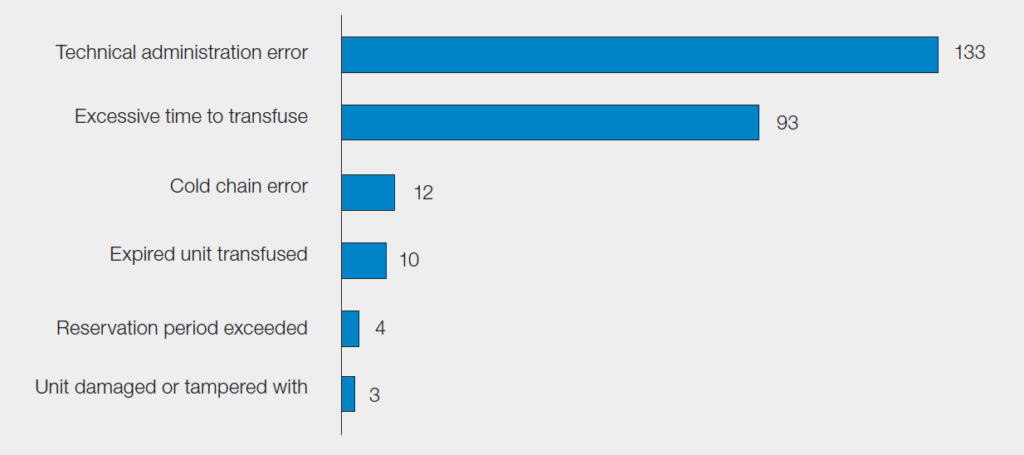
The number of clinical errors has seen a slight increase from 241 in 2024 to 255 in 2025 and
there has been a larger percentage increase in technical administration errors, 133/255 (52.2%) in 2025 compared to 103/241 (42.7%) in 2024.
Figure 11.2: Breakdown of clinical HSE by category in 2025 (n=255)
Technical administration errors n=133
Technical administration errors have been further categorised in Table 11.1.
Table 11.1: Clinical technical administration errors (n=133)
| Technical administration error | Number of cases |
| Setting an infusion pump incorrectly or equipment failure | 87 |
| Use of an inappropriate giving set | 32 |
| Co-administration of a blood component and drug through the same venous access | 6 |
| Administered too quickly (manual) | 5 |
| Administration of two units simultaneously in a non-urgent situation | 2 |
| Transfusion of a component which has had a drug added | 1 |
| Total | 133 |
There were 87 pump errors and 80 were due to user error. Of these 80, there were 76 that had the
correct prescription/authorisation, but the pump had been set incorrectly. There were 6 errors due to
pump equipment failure that included pumps infusing too quickly or too slowly even though they were set correctly. In one pump error case, it was suspected that the patient may have altered the rate. Pump errors also resulted in 3 overtransfusions and 15 undertransfusions, which are included in Chapter 14, Under or Overtransfusion.

There were 32 giving set errors reported and 25/32 (78.1%) were due to the incorrect giving set
being used, see Case 26.8 in Chapter 26, Paediatric Cases. There were 7 errors reported that were a
combination of cannula position and clamp errors. The MHRA have released a Device Safety Information (DSI/2026/003) notice highlighting the risk of serious patient harm when standard IV administration sets are mistakenly used for blood transfusions (see ‘Recommended resources’).
Excessive time to transfuse errors n=93
Of the 93 excessive time to transfuse errors reported, 44 involved inefficient written or verbal
communication that contributed to the error and 48 stated that handover between shifts, teams, or
individuals impacted the error. Transfusions were classed as routine in 52/93 and 36 of these were within normal working hours. There were 32/93 classed as urgent transfusions with 21 of these taking place outside of normal working hours.
Case 11.1: Transfusion set up and running for approximately 19 hours
A unit of red cells was removed from temperature-controlled storage at 10:19 and the transfusion was commenced at 10:45. The patient was moved to a different ward while the transfusion was in progress and handed over to a member of staff. At 19:45 the night shift noticed that the blood had stopped transfusing but were unsure how long for and started it running again. The transfusion completion time was not recorded but a post-transfusion blood gas was run at 05:44 the next morning.
On investigation the unit had been transfusing for 9 hours when the night shift restarted it and as no completion time was recorded it could have been transfusing until the post-transfusion blood gas was run, meaning the unit had been out of temperature-controlled storage for over 19 hours.
The three nurses involved also had not completed the training and competency assessments to administer blood or care for a patient who is receiving a blood transfusion.
Learning points
- Staff must be trained and competent to administer blood transfusions.
- Clear communication between shifts and during handover is essential to ensure that transfusions are managed appropriately.
Laboratory errors n=68
The number of laboratory errors have decreased slightly to 68 in 2025 from 70 in 2024 and are illustrated by HSE category in Figure 11.3. The majority were cold chain errors, 41/68 (60.3%) which have been further categorised in Table 11.2.
Figure 11.3: Breakdown of laboratory HSE by category in 2025 (n=68)
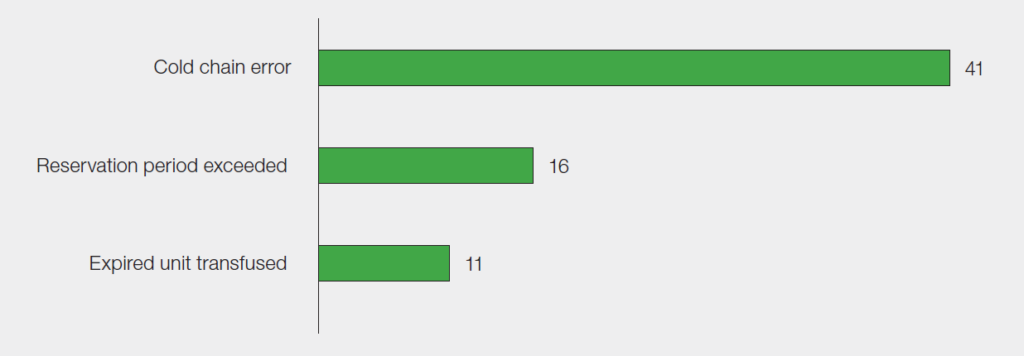
Table 11.2: Laboratory cold chain errors (n=41)
| Cold chain error | Number of cases |
| Inappropriate return to stock | 22 |
| Refrigerator or equipment failure | 8 |
| Incomplete cold chain | 6 |
| Transport and delivery | 5 |
| Total | 41 |
Inappropriate return to stock errors have doubled compared to 2024, of which 21/22 (95.5%) involved
information technology (IT). The reasons included systems not being used correctly, lack of functionality or algorithms to support safe practice, lack of interfacing or interoperability and warning flags in place but not heeded. In addition, 11/21 identified that the staff member was lone working at the time of the error, illustrating the importance of safe IT systems to support transfusion practice.
The number of refrigerator or equipment failures has decreased substantially to 8/41 in 2025 compared to 20/47 in 2024. This could be the result of actions taken in hospital laboratories in line with the learning point from the 2024 HSE chapter that laboratory standard operating procedures (SOP) should be clear and give clear instructions on how to deal with any system alerts or alarms generated.
Case 11.2: Transfusion of a component that was out of temperature control
The Helicopter Emergency Medical Services team attended a trauma patient and transfused
three of the four units of fresh frozen plasma (FFP) from the sealed temperature-controlled box at approximately 19:45. The opened box containing the remaining one unit of unused FFP was then returned to the transfusion laboratory at 22:45. The unit of FFP was electronically returned to stock at 00:01 the next day. At this point, the unit should have been discarded, but this action was not undertaken. There was also no record of the unit being placed into the stock refrigerator after being electronically returned to stock (in line with local procedure). This suggests that it was left out on the bench at room temperature in the laboratory. It was later issued to another patient at 01:56, and transfused at 02:21 after being out of temperature-controlled storage for approximately 6 hours.
The investigation identified that there was miscommunication between laboratory staff regarding disposal of the FFP. The patients’ notes were reviewed and there was no indication of harm.
Learning points
- Clear laboratory SOP on how to handle units returned to the laboratory, including quarantining and disposal, help prevent handling and storage errors.
- Appropriate configuration of laboratory information management systems/electronic blood management systems prevent the inappropriate return to stock of blood components.
Near miss (NM) HSE n=129
There were 129 NM HSE events in 2025, including 105/129 (81.4%) clinical errors and 24/129 (18.6%)
laboratory errors. Clinical errors were mainly due to cold chain errors, 99/105 (94.3%), where units were stored in inappropriate conditions in the clinical area, 75/99 (75.8%). Laboratory errors were mainly due to expired units issued, 13/24 (54.2%), 4 cold chain errors and 4 reservation period exceeded.
In 49/129 (38.0%) cases, the error was detected due to staff diligence and awareness of the correct
procedure and highlighting the discrepancy. Other detection routes included the use of a pre-administration checklist (23), issue detected when unit was returned to the laboratory (20), detected by laboratory staff after collection (14), and on arrival receipt of unit to the clinical area (4).
Conclusion
HSE remain consistent with previous years’ Annual SHOT Reports. Gaps in written and/or verbal
communications during the handover between shifts or teams and in knowledge and training in both
clinical and laboratory environments are all being reported. All laboratory and clinical staff who are involved in the handling and storage of blood components, must be fully trained and competent to do so. The correct procedures that are outlined in national guidance should be contained within local transfusion policies and reflected in the relevant staff transfusion training requirements.
Recommended resources
Safe blood administration toolkit
Patient Blood Management – Blood Assist app also available at App marketplaces (App Store and Google Play)