Authors: Josephine McCullagh, Paula Bolton-Maggs, and Vera Rosa
Link to PDF chapter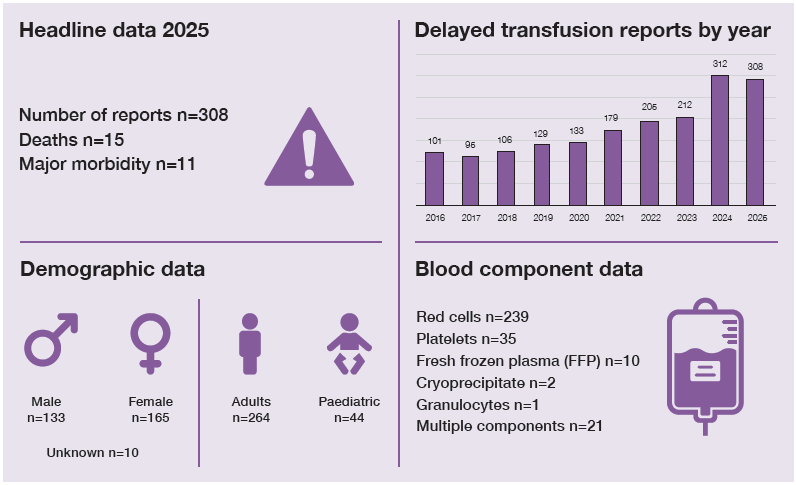
Key SHOT messages
Key findings
- The number of transfusion delays remains high with 15 cases resulting in death and 11 cases of major morbidity, mainly in urgent and emergency settings.
- Communication gaps were the most common contributory factor across all transfusion priorities.
- Major haemorrhage (MH) cases highlight recurrent, multifactorial system failures.
Gaps identified
- Communication issues were the most frequently cited factor, affecting decision-making, blood component requests, and sample processing.
- Lack of training, understaffing, and unfamiliarity with emergency protocols significantly impacted transfusion response times in both clinical and laboratory areas.
Good practice
- Increased levels of recognition and awareness of delays resulting in reporting of such events.
- Increasing acknowledgement of causal and contributory factors that can help improve safety.
Next steps
- Utilise the resources of the SHOT Major Haemorrhage Simulation Toolkit to improve safety and readiness when managing MH.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Delayed transfusion definition
Where a transfusion of a blood component was clinically indicated but was not undertaken or
non-availability of blood components led to a significant delay (e.g., that caused patient harm,
resulted in admission to ward, or return on another occasion for transfusion).
For a more detailed definition see SHOT Definitions
Introduction
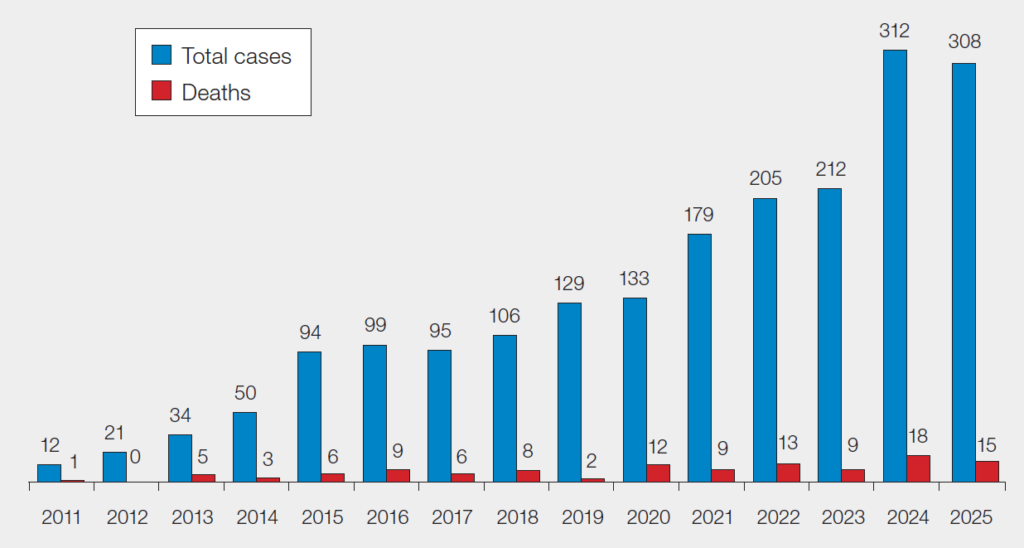
Reports of delays in transfusion continue to be a significant patient safety concern. Despite the publication of a Central Alerting System (CAS) patient safety alert outlining actions for hospitals (SHOT, 2022), the number of delays reported to SHOT remains worryingly high (Figure 12.1). In 2025, a total of 308 delays were reported, with 15 associated deaths and 11 cases of major morbidity. These figures are concerning and highlight the ongoing serious risk to patients when timely transfusion is not achieved.
As in previous years, delays in transfusion are rarely attributable to a single point of failure. Rather, they typically arise from a combination of system, process, and human factors that collectively contribute to delays in patient care. Recurring themes identified in earlier reports, including ineffective communication, delayed recognition of bleeding, and gaps in knowledge and training, continue to feature prominently in this year’s analysis. The persistence of these issues highlights the need for sustained focus, organisational learning, and effective implementation of existing safety recommendations to reduce harm from transfusion delays.
Figure 12.1: Delayed transfusions by year 2011-2025
Deaths related to transfusion n=15
There were 15 deaths reported due to delays. This compares with 18 deaths related to delays in 2024
and 9 in 2022. The majority (n=11) were associated with delays in urgent or emergency transfusions.
Common themes were delays in recognition of bleeding and miscommunication.
- 6 probably related (imputability 2)
- 9 possibly related (imputability 1)
Of all the deaths associated with delays in transfusion, 13 were related to clinical errors and 2 were related to laboratory errors. Most of the delays affected patients who were actively bleeding (n=9). Common themes identified were miscommunication (n=7), a delay in recognising bleeding in the patient (n=6), component collection processes not being followed (n=1) and equipment failure (n=1).
Case 12.1: Multiple issues in communication contributes to the death of a critically ill newborn baby (imputability 1 – possible)
A full-term woman underwent an emergency caesarean section for placental abruption. The baby was born profoundly pale and in poor condition. Red cells were urgently requested. Although urgency was communicated to the laboratory, the O D-negative units available in the theatre refrigerator were not used. An adult O D-negative unit was authorised and issued within 5 minutes; however, delays occurred as the staff member transporting the unit had no access to theatres and had to wait for entry. On arrival, the baby had been transferred to the special care baby unit, which had not been communicated between teams, causing further delay while access was gained. Red cells were transfused approximately 25 minutes after the request. A second unit was later requested and transfused. Despite transfusion and resuscitation, the baby died later that evening.
Case 12.2: Inadequate communication results in delayed blood provision for an elderly patient with red cell antibodies (imputability 2 – probable)
A patient with known myeloma was admitted to the emergency department, which was severely overcrowded, with extensive corridor care. They had a significantly low haemoglobin and red cell antibodies, and compatible blood was requested from the Blood Service. Once the compatible blood was received in the laboratory, its availability was not communicated to the clinical team. While waiting for blood, the patient fell, became unresponsive and suffered a cardiac arrest. During resuscitation, one unit of emergency O D-positive red cells was administered; however, resuscitation was unsuccessful.
This case is discussed in further detail in Chapter 18, Laboratory Errors, Case 18.1.
Major morbidity n=11
There were 11 cases that resulted in major morbidity due to delays. This compares with 12 in 2024.
Delays in recognising bleeding, technical information technology (IT) issues and sampling errors were
the most common reasons identified.
Case 12.3: Lack of knowledge of MH protocol contributes to the harm of an obstetric patient
The obstetric MHP was activated in maternity theatres for a patient with placental abruption. Confusion arose regarding whether fresh frozen plasma (FFP) was included in MH packs. An outdated protocol, which included FFP in standard packs, remained displayed in theatres despite an update removing FFP from packs and directing staff to a rotational thromboelastometry (ROTEM)-guided pathway. As a result, FFP was not requested when indicated, leading to a 28-minute delay. The patient suffered a seizure and rapidly deteriorated due to haemorrhage and disseminated intravascular coagulation. Leadership and communication challenges were noted. At the time of submission, the investigation
into patient harm was ongoing.
Reason for delays n=308
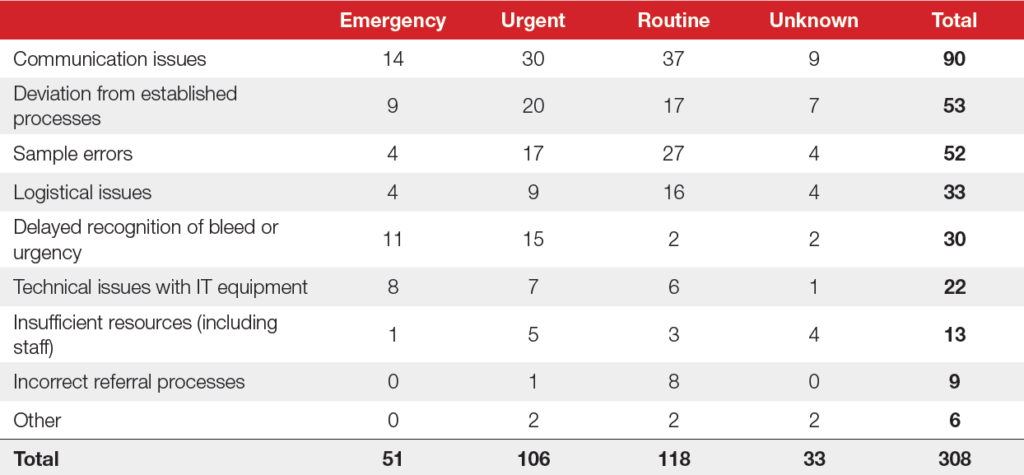
Table 12.1 summarises the main contributory factors associated with transfusion delays reported in 2025, divided into priority of transfusion request. Delays were most frequently reported in routine (n=118) and urgent (n=106) transfusions, with 51 emergency delays also identified.
Across all transfusion priorities, communication issues were the most reported contributory factor,
particularly in routine and urgent cases. These included breakdowns in communication between
clinical teams and transfusion laboratories, unclear escalation pathways, and delays in relaying critical information. Deviation from established processes was the second most frequently reported factor highlighting ongoing challenges with adherence to transfusion policies and procedures.
The distribution of contributory factors across all transfusion priorities shows that delays arise from a
combination of clinical, laboratory, and organisational factors. Addressing these requires coordinated
system-wide approaches, with particular focus on improving communication, strengthening process
effectiveness, and ensuring adequate resources to support timely transfusion care.
Table 12.1: Primary reason for transfusion delay in 2025 (n=308)
Laboratory errors n=82
The number of laboratory errors that resulted in delays were fewer in 2025 than in the 2024 Annual
SHOT Report (n=120), but up from the 2023 Annual SHOT Report (n=56). Communication issues
and deviation from the correct procedure were the most common problems identified. The availability of blood components was a key step in the transfusion pathway where errors occurred. Inadequate communication between clinicians, transfusion laboratories, and porters or couriers frequently led to delays in decision-making and blood availability.
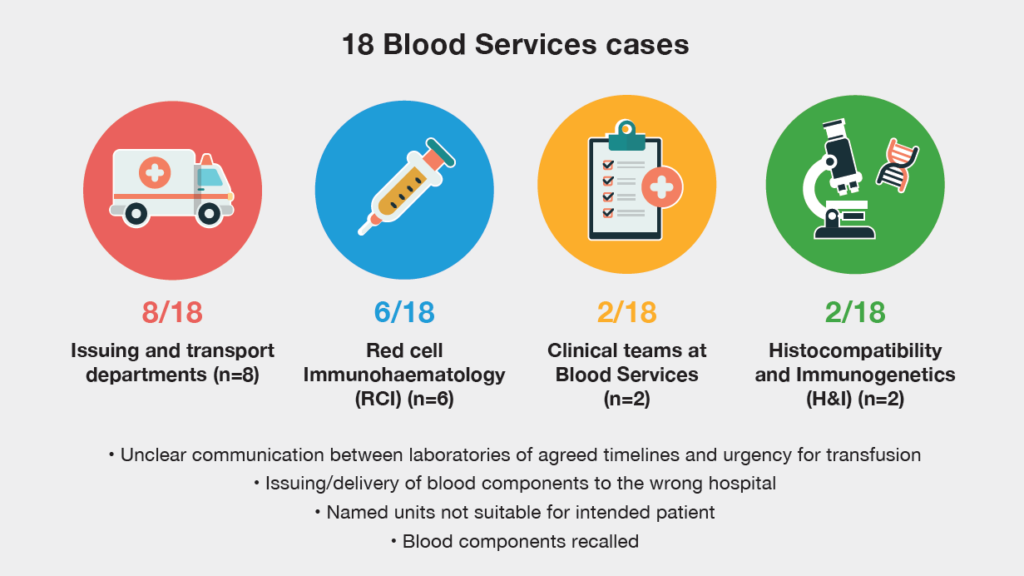
Blood Service errors n=18
There were 18 reports of delayed transfusions reported by hospitals related to errors from the Blood
Services in the UK. Details of these cases are shown in Figure 12.2.
Figure 12.2: Reason for delays in blood transfusion and location of errors associated with
Blood Services in 2025 (n=18)
To strengthen haemovigilance monitoring, learning from and improving transfusion safety across the
system, the Blood Services in the UK began reporting to SHOT in August 2025. This is a new process,
and the project was initially launched with 4 reporting categories, which may expand in future to include for example delayed transfusions. Further information about this collaborative project, reporting categories and cases submitted by the Blood Services can be found in the relevant chapter of this report: Chapter 7, United Kingdom (UK) Blood Services Reporting.
Delays associated with MH n=42
Issues associated with MH continue to be a major contributor to delays (Figure 12.3). Although 2025
has seen a reduction in overall reports of delays during MH (2024 n=73), there has been an increase in
the proportion of these cases resulting in serious patient harm; 8/42 (19.1%) resulted in death and 5/42 (11.9%) resulted in major morbidity. Several recurring themes continue to be raised in this year’s Annual SHOT Report, highlighting the systemic, procedural, and logistical issues contributing to delays in blood transfusion during MH cases (Figure 12.4). These high-pressure, time-sensitive scenarios reveal that each case is not simply a result of a single error but rather a multitude of factors resulting in delayed care.
Figure 12.3: Delays associated with MHP 2016-2025, including the proportion of reports
resulting in mortality or major morbidity
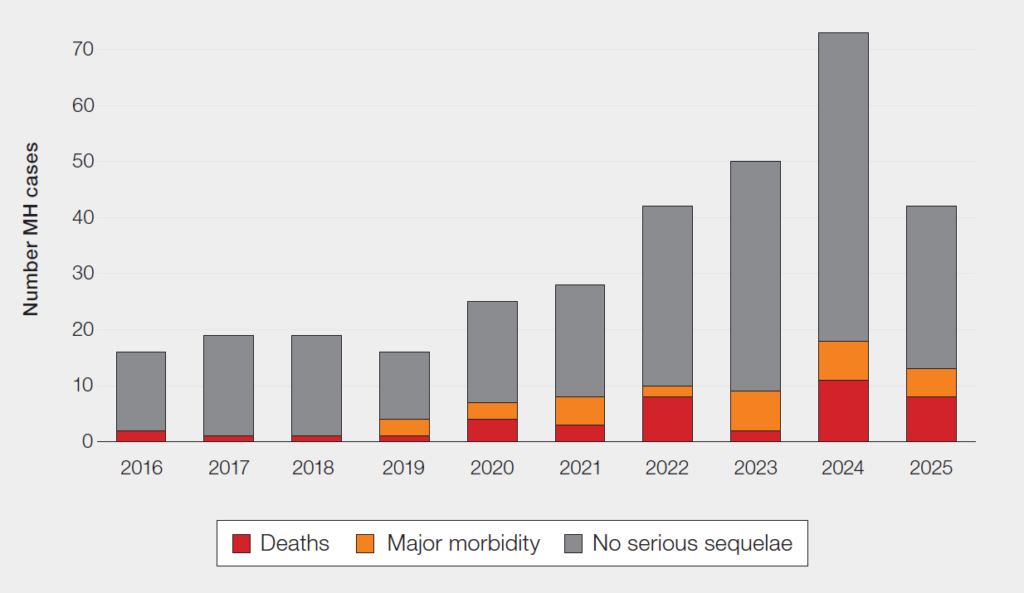
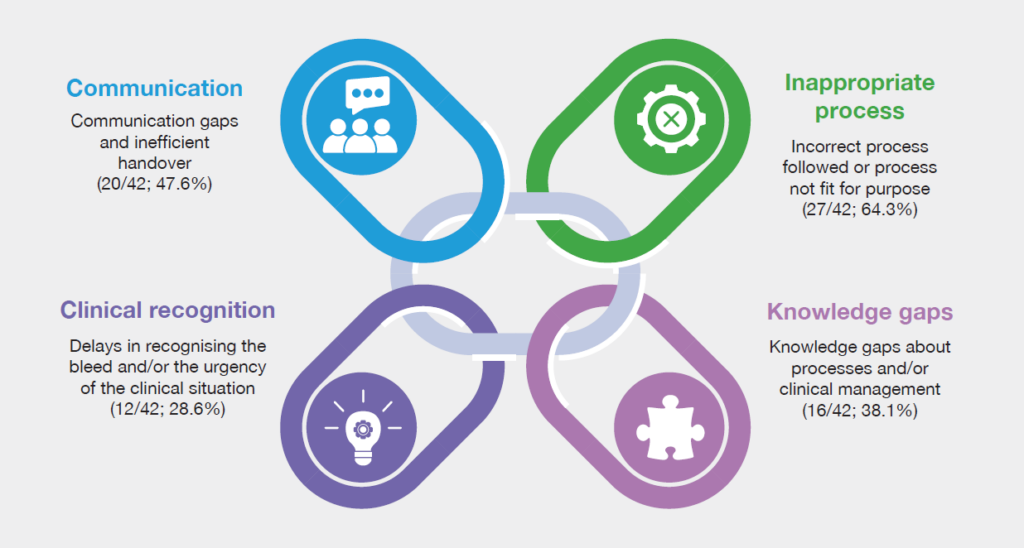
Figure 12.4: Common themes identified that contributed to delays during MH in 2025
Learning points
- All clinical and laboratory staff working in transfusion must have adequate knowledge and skills to ensure safety.
- Prompt recognition of bleeding is crucial for timely and appropriate treatment.
- Awareness of contingency plans is essential to ensure smooth processes when technical issues arise.
- Clear protocols should be in place to support healthcare staff when requesting and issuing blood components in emergency situations, especially for patients with red cell antibodies.
Near miss delayed transfusion n=1
This case involved difficulties in contacting the transfusion laboratory during a MH situation. A review of the event resulted in the installation of a second telephone line in the laboratory.
Conclusion
Patients should not die or suffer harm as a result of transfusion delays. The continued occurrence of
deaths and cases of major morbidity associated with delayed transfusion in 2025 remains a serious
concern. Persistent contributory factors including communication issues, gaps in clinical knowledge,
and workforce pressures continue to be key drivers of harm. Urgent and sustained action is required to improve transfusion safety, particularly during major haemorrhage and emergency situations.
Any delay in initiating a clinically necessary blood transfusion has the potential to cost lives. Timely
transfusion support is a critical, life-saving intervention. All systems, processes, and staff involved in
transfusion care must prioritise rapid access to blood components to reduce the risk of avoidable harm or death.
Reliable and safe transfusion IT systems are vital to patient safety. System failures, delays, or design
limitations can compromise timely transfusion and place patients at risk. Continued attention and
investment are needed to ensure transfusion IT systems are robust, effective, and resilient.
The SHOT CAS alert provides clear recommendations to mitigate the risks associated with transfusion
delays (SHOT, 2022). Effective implementation depends on addressing challenges related to staffing
capacity, education and training, and communication pathways within transfusion laboratories and across clinical services. The recently published Major Haemorrhage Simulation Toolkit provides a structured framework to support the implementation of MH simulation, a CAS alert action. Sustained commitmentin these areas is essential to support improvement and reduce the risk of future harm.
Recommended resources
SHOT Bite No.08: Massive haemorrhage – delayed transfusion
SHOT Video: Delayed Transfusions in Major Haemorrhage
Major Haemorrhage (MH) Simulation Toolkit
