Authors: Catherine Booth, Paula Bolton-Maggs and Vera Rosa
Link to PDF chapter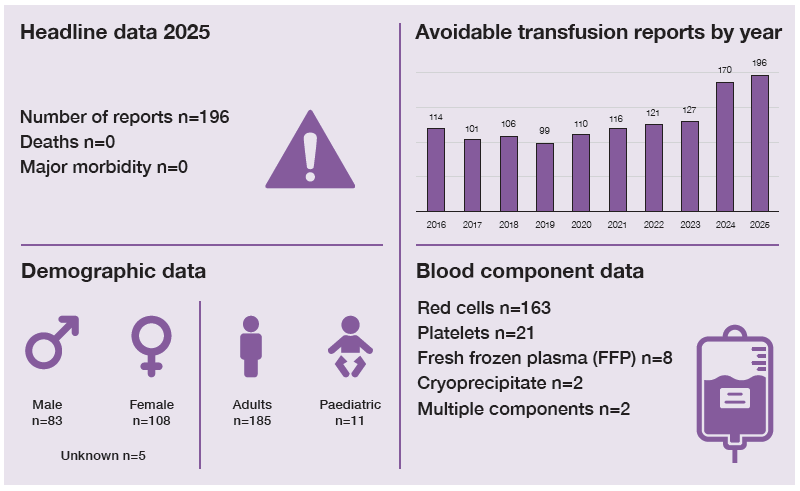
Key SHOT messages
Key findings
- There has been an increase in reports of avoidable transfusions compared to 2024
- The largest rise in reports related to flawed decisions and avoidable use of emergency group O red cells.
- There were 135 transfusions that might have been completely avoidable.
Gaps identified
- Clinician knowledge of appropriate anaemia management for haematinic deficiencies.
- Ineffective communication of results, decisions and component availability.
- Lack of timely and accurate group and screen sampling in patients presenting with bleeding or with potential need for transfusion.
Good practice
- Evidence of avoidable transfusions minimised following challenges by nursing, laboratory and other medical staff.
- In-depth local investigations providing insight into a range of contributory factors.
Next steps
- Feed back avoidable transfusions to clinical teams as learning opportunities and ensure tools to support decision-making are readily available in clinical areas.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Avoidable transfusion definition
A dose inappropriate for the patient’s needs, excluding those cases which result in transfusion-associated circulatory overload (TACO) and usually resulting in a haemoglobin or platelet level
significantly outside the intended target range. Infusion pump errors leading to under or over
transfusion with clinical consequences (if no clinical consequences, then it is reportable under
handling and storage errors (HSE)).
For a more detailed definition see SHOT Definitions
Introduction
The 196 reports of avoidable transfusions in 2025 continues the upward trend of previous years. The
increase was driven by additional reports related to flawed decisions and avoidable use of emergency
group O. This is likely to reflect increased awareness and vigilance from transfusion teams. The challenge is disseminating this same awareness to clinical staff.
There were 135 transfusions that might have been avoided entirely (compared to 124 in 2024). In
addition, there were 61 reported cases of avoidable use of emergency group O red cells (46 in 2024).
Deaths or major morbidity related to transfusion n=0
No cases reported in the avoidable transfusion category resulted in death or major morbidity.
However, some deaths or cases of major morbidity reported in other chapters (e.g. transfusion-associated circulatory overload (TACO) or febrile, allergic or hypotensive reactions (FAHR)) were the result of potentially avoidable transfusions.
Classification of avoidable transfusions
Table 13.1: Classification of avoidable transfusions
| Group | Red cells | Platelets | Plasma components | Multiple components | Total reports |
| Flawed decision | 39 | 14 | 9 | 1 | 63 |
| Decision based on inaccurate results | 43 | 5 | 1 | 1 | 50 |
| Failure to respond to change in circumstances | 9 | 2 | 0 | 0 | 11 |
| Transfusion without decision | 8 | 0 | 0 | 0 | 8 |
| Transfusion necessitated by error | 3 | 0 | 0 | 0 | 3 |
| Sub total | 102 | 21 | 10 | 2 | 135 |
| Avoidable use of emergency group O | 61 | 0 | 0 | 0 | 61 |
| Grand total | 163 | 21 | 10 | 2 | 196 |
Flawed decision n=63
These included 32 patients transfused outside of guideline thresholds, 13 patients unnecessarily
receiving multiple units, 12 avoidable transfusions for haematinic deficiency (10 iron, 2 B12/folate), and 3 transfusions in patients with sickle cell disorder without a clinical indication. All of these were due to gaps in knowledge. In addition, there was 1 case related to inaccurate estimation of bleeding and 2 patients transfused despite withholding their consent.
Case 13.1: Multiple units transfused for anaemia due to B12 and folate deficiency
A patient with severe anaemia (haemoglobin (Hb) 29g/L) due to profound B12 and folate deficiency, who was moderately symptomatic but stable, was transfused seven units of red cells in the medical assessment unit. Post-transfusion Hb was 86g/L. It was noted that the patient presented overnight, resulting in decisions being made without senior or specialist input. Shift handovers did not clearly highlight the reversible cause for the chronic anaemia.
Decision based on inaccurate result n=50
These included 17 haemodiluted samples, 15 erroneous laboratory results, 7 inaccurate results from
blood gas machines, 4 old results, 4 cases where results were misread or handed over incorrectly and
3 cases of wrong blood in tube for the full blood count (FBC).
Case 13.2: Missed opportunity to review a decision to transfuse based on a haemodiluted sample
A Hb result of 67g/L was telephoned through for a patient on the surgical assessment unit. A
consultant told a resident doctor to authorise two units of red cells. A venous blood gas taken an hour later gave a Hb of 96g/L, in keeping with the patient’s baseline. The resident doctor filed these results but did not question the transfusion decision. During transfusion of the second unit, a nurse noticed the blood gas result and queried the discrepancy with the out-of-hours biomedical scientist. The transfusion was paused whilst a repeat FBC was performed. The repeat Hb was 110g/L. The original FBC sample was found to have been taken from the same arm that had intravenous fluids running.
Learning points
- Results that are not in keeping with the clinical picture should be questioned, particularly where there is a marked change from previous values. Unless there is clinical urgency, repeat samples should be taken before deciding to transfuse.
- Creating a culture where decisions are open to discussion and challenge can help all staff (resident doctors, nurses, laboratory staff) to feel able to question transfusion plans.
Failure to respond to change in circumstances n=11
There were 4 cases where components ordered ‘just in case’ were transfused routinely, 4 prescriptions/ authorisations written in advance for regularly transfused/day unit patients whose latest results were not checked, 2 changes in treatment plan not communicated and 1 patient who had received iron and had no repeat Hb check to assess the need for transfusion.
Case 13.3: Change in plan for an iron infusion rather than blood transfusion in pregnancy not communicated
A pregnant woman reported tiredness and was found to have a Hb of 88g/L. A blood transfusion was initially planned, but this was changed to an iron infusion following medical review after haematinic results were available. This was not communicated to the midwife, although the plan was documented. The notes were not checked at the change of shift, and a unit of red cells was transfused. Two units had originally been requested, but this was reduced to one after challenge by the laboratory.
Learning points
- Transfusion should only be given in the context of haematinic deficiencies when the anaemia is severe, and the patient has significant symptoms or there is a risk of decompensation. The minimum volume to achieve clinical stability should be given. There is a high risk of TACO in this scenario.
- There is a risk of errors during verbal handover. Written plans and patient results should be checked wherever possible.
Transfusion without decision n=8
These included 3 patients transfused based on a prescription/authorisation written in error (should have been for another patient), 2 patients had no prescription/authorisation, and 3 received multiple units which had been ordered but not all were prescribed/authorised or intended. Verbal handover was a common factor.
Case 13.4: Lack of training in electronic systems resulted in an avoidable transfusion based on a verbal handover
Two units of red cells were crossmatched for a patient presenting with a suspected ectopic
pregnancy, in preparation for possible surgery. The Hb was 116g/L. One unit was administered on the ward following a verbal handover from an emergency department (ED) nurse. None of the ward staff were trained to use the electronic blood tracking system and a nurse was called from another ward to start the transfusion. Staff did not know where to locate the prescription/authorisation on the electronic patient record and were therefore unaware that one had not been completed.
Transfusion necessitated by error n=3
These 3 cases all related to inadequate management of iron deficiency (2 in pregnancy), resulting in
blood transfusion being required at the time of surgery.
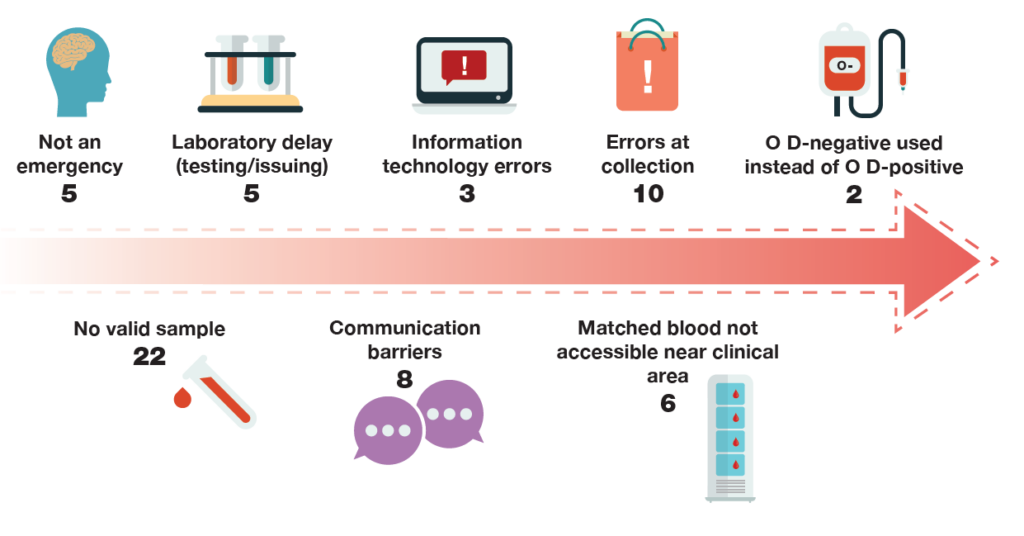
Avoidable use of emergency group O n=61
Errors can occur at any point in the transfusion pathway leading to avoidable use of emergency group
O. The number of reports related to key points is illustrated in Figure 13.1. The largest category involved delays in sending group and screen samples, or where samples were rejected due to mislabelling. It should be noted that reverting to emergency group O in this scenario is appropriate, to avoid patient harm from delay to a necessary transfusion, however this could have been avoided had a sample been available.
Figure 13.1: Errors during the transfusion pathway resulting in avoidable use of emergency
group O (n=61)
Case 13.5: Delay in taking a group and screen in a patient with gastrointestinal bleeding results in the avoidable use of emergency group O
An elderly male presented to the ED with haematemesis. No group and screen sample was taken at the primary assessment. Six hours later, it was noted he had ongoing haematemesis, but no blood tests were taken at that time. A further two hours later, he deteriorated and was transfused with a unit of emergency group O. The first transfusion sample was only taken after this. In addition, group O D-negative was selected when he could have received O D-positive. It was noted that staff numbers in the ED were insufficient for the volume of patients received.
Learning point
- Patients with high potential to need transfusion (e.g. presenting with bleeding or an acute surgical problem) should have transfusion samples taken as part of their initial assessment.
Near miss avoidable transfusions n=6
There were 6 cases where an avoidable transfusion was prevented in 2025. All cases were in the clinical area and included 2 instances of the wrong results being reviewed; reticulocyte count instead of platelet count in 1 case, and blood sugar results instead of haemoglobin in the other. The remaining cases involved platelets being ordered for the wrong patient, a unit almost being administered without a Hb check, an O D-negative unit being collected instead of a fully crossmatched unit, and finally a unit that was almost transfused to prevent wastage.
Conclusion
All staff have a role to play in ensuring transfusion is only given when there is a clear indication. The
decision must be informed by sound clinical assessment, judgement and guidelines, based on accurate laboratory results, and plans correctly executed. High-quality consent discussions and involvement of patients in shared decision-making can provide a further opportunity to scrutinise the recommendation to transfuse and ensure all alternatives have been fully explored.
Cases where transfusion could have been avoided should be fed back to the teams directly involved
but also shared more widely as learning opportunities.
UK Blood Services saw a severe shortage of group O red cells throughout 2024, and although this
eased in 2025, ongoing high demand means the stock situation remains delicately balanced. Ensuring
wise use of emergency group O should still be a priority, and the increasing number of reports in this
category confirms this issue remains a focus for transfusion teams.
Recommended resources
SHOT Bite No.34 Switching to group specific red cells during major haemorrhage (MH)
Major haemorrhage simulation toolkit
National Blood Transfusion Committee indications codes for transfusion (updated 2024)