Authors: Paula Bolton-Maggs and Vera Rosa
Link to PDF chapter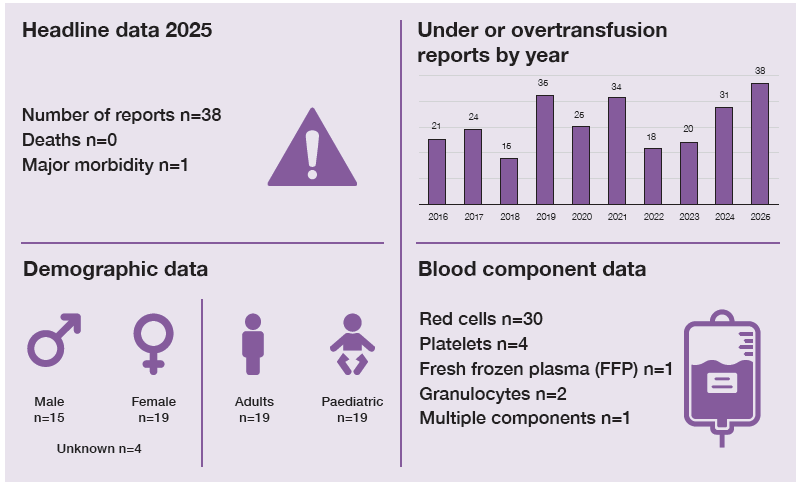
Key SHOT messages
Key findings
- Paediatric cases made up half of all reports of under and overtransfusion.
- Errors with pump settings and infusion rates are common.
Gaps identified
- Programming of infusion pumps at the wrong rate or the wrong total volume.
- Environmental factors can lead to equipment errors, for example insufficient lighting.
- Knowledge gaps surrounding granulocytes dosing and requesting resulted in undertransfusion; standard doses come as two units.
Good practice
- Investigations showed appropriate corrective and preventive actions, including shared learning.
- Examples of prompt action and escalation following identification of under- and overtransfusions, which led to improved patient outcomes.
- Involvement of parents at each stage of the investigation for a paediatric undertransfusion error.
Next steps
- Include guidance on how to calculate the volume and rate required in policies for paediatric and neonatal transfusions.
- Ensure staff have sufficient knowledge on how to programme infusion pumps correctly.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Under or over transfusion definition
A dose inappropriate for the patient’s needs, excluding those cases which result in transfusion-associated circulatory overload (TACO) and usually resulting in a haemoglobin or platelet level
significantly outside the intended target range. Infusion pump errors leading to under or over
transfusion with clinical consequences (if no clinical consequences, then it is reportable under
handling and storage errors (HSE)).
For a more detailed definition see SHOT Definitions
Introduction
There were 38 cases in total, of which 20 related to issues with pumps or rates of infusion (15 resulted
in undertransfusion and 5 in overtransfusion). Paediatric cases made up 19/38 (50.0%), including 5 with haemoglobin disorders. Overall, the majority, 37/38, were due to clinical errors.
Deaths related to transfusion n=0
There were no deaths as a result of under or overtransfusion in 2025.
Major morbidity n=1
A patient received a transfusion over 30 minutes resulting in admission to the intensive care unit (ICU)
(Case 14.1).
Overtransfusion n=18
In 3 patients, 2 with major haemorrhage and 1 acute gastrointestinal bleed, more red cells were
administered than necessary. In an emergency the extent of blood loss may be difficult to assess. Regular checks on the haemoglobin (Hb) (including point-of-care tests (POCT)) can help to avoid overtransfusion.
A patient with chronic anaemia due to cancer treatment, weight 47kg, was prescribed 188mL and was
transfused a whole unit (288mL) but came to no harm.
An infant received an excessive red cell transfusion volume when a POCT measurement of Hb was
misheard as 116g/L but the correct result was 160g/L.
Errors in prescription/authorisation n=8
Where there was an error in prescription/authorisation, 7 cases involved paediatric patients, of which 2 were on regular transfusions for thalassaemia. In another case where preoperative transfusion occurred, two units were each given over 1 hour instead of 3 hours. The anaesthetist changed the prescription/authorisation to ensure the top-up occurred before surgery on the same day for a fractured neck of femur.
Errors in infusion equipment n=5
There were 5 errors due to infusion equipment; 3 due to pump errors and 2 due to infusion errors, which are described in Case 14.1 and Case 14.2.
Case 14.1: Rapid transfusion followed by respiratory compromise
A young patient with a history of renal transplantation and continued renal dysfunction was admitted with abdominal pain and prescribed a single-unit red cell transfusion. This was infused over 30 minutes instead of 3 hours. Eight hours later, the patient developed haemoptysis and desaturated, necessitating admission to the ICU. Chest X-ray changes favoured infection rather than fluid overload. The patient received furosemide without obvious benefit. Criteria for TACO were not met, and the patient made a full recovery.
Case 14.2: Dim light associated with wrong infusion settings
A small child was transfused an excessive volume of red cells (327mL) resulting in a Hb rise from 82g/L to 169g/L. The prescribed volume was 150mL over 4 hours. The parents had requested the child not be disturbed, so the transfusion was set up in dim light and not checked later at staff changeover.
Undertransfusion n=20
In 15 cases the infusion was given at the wrong rate or there were problems with the pump settings
(including battery failure); 6 were paediatric cases. Most related to red cells but 2 patients did not receive their intended dose of granulocytes (2 bags) as the second bags were not infused (one of these was a laboratory error). One adult only received a single unit of FFP which was an inadequate dose.
Learning point
- Infusions using pumps should be carefully set up, and the electricity supply should be confirmed to be adequate to ensure the patient receives the intended quantity of the transfusion.
Conclusion
Over or undertransfusion is more likely to occur in paediatric patients and where infusion pumps are
incorrectly set or used. Gaps in knowledge and understanding of paediatric and neonatal transfusion
volume calculations in line with national guidance continue to impact patient and transfusion safety.
Transfusion of the incorrect rate or volume can lead to serious consequences, impacting on patient
wellbeing. Overtransfusion can be a contributory factor in cases of TACO, as discussed in Chapter 21a.
Recommended resources
Avoidable, Delay and Under or Overtransfusion (ADU) Cumulative Data
Avoidable, Delayed or Under/Overtransfusion webinar (ADU)
SHOT Bite No.4: Lessons in Paediatrics (including neonates)