Authors: Paula Bolton-Maggs, Vera Rosa and Niamh Reynaud
Link to PDF chapter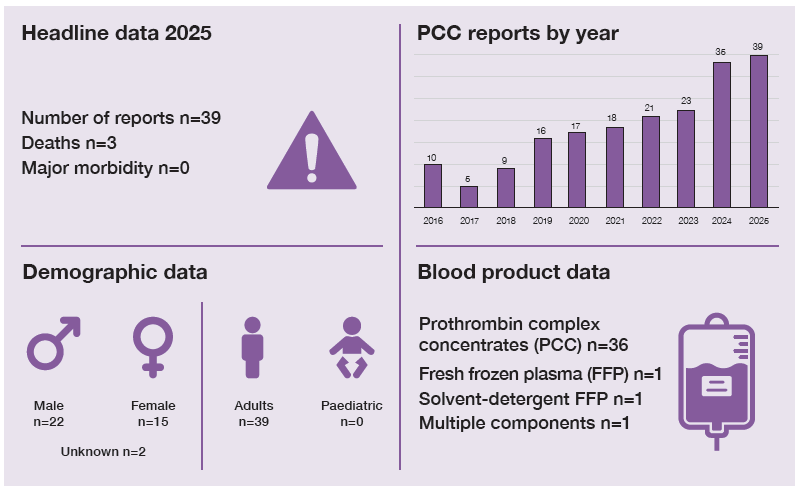
Key SHOT messages
Key findings
- Delays remain the main reason for PCC reports, 23/39 (59.0%).
- Most patients were elderly (74.4% aged >70), with intracranial haemorrhage (ICH) common in this group.
- Most events occurred in clinical areas, 35/39 (89.7%).
Gaps identified
- Uncertainty about local policy for dose, stock location, ordering, and administration contributes to delays.
- Failure to recognise clinical urgency and bleeding risk in patients receiving anticoagulants.
Good practice
- Retrospective audits of PCC usage and major haemorrhage protocols (MHP) identified PCC incidents, which may lead to improved processes in the future.
Next steps
- Protocols for anticoagulant reversal should be accessible and include how to prescribe, order, and administer PCC.
- Rapid release of a fixed dose PCC in the emergency department (ED) should be considered, with follow up international normalised ratio (INR) for patients on warfarin to ensure adequate correction.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
PCC definition
Delays in administration, inappropriate prescription, or problems with administration related to PCC infusion. Allergic reactions should be reported to the Medicines and Healthcare products Regulatory Agency (MHRA) through the Yellow Card scheme.
For a more detailed definition see SHOT Definitions
Introduction
Delays in treatment with PCC occurred in 23/39 (59.0%) cases. Avoidable use of PCC was reported in
5 cases. The patient age range was 39 to 103 years with the majority, 29/39 (74.4%), >70 years of age.
The median age was 80 years. There were 22 cases with ICH, including 18 with a delay in treatment.
Most cases, 35/39 (89.7%) originated from clinical areas.
In 14 of 39 cases, a knowledge gap contributed to the error. Two patients received less than the
recommended dose and 8 received more than recommended. Both available brands of PCC have an
upper limit for dosing, and this should be adhered to.
Deaths related to transfusion n=3
There were 3 deaths related to delayed PCC infusion (1 possibly, and 2 probably related). These 3
patients all had ICH, 2 were over 90 years of age: 1 possibly related had a delay of 5 hours (Case 15.1),
and 2 cases probably related had delays of 8.5 (Case 15.2) and 7.5 hours.
Major morbidity n=0
One patient suffered a cerebrovascular event within 48 hours of anticoagulant reversal (details in the
supplementary material) but it was not considered to be related to the PCC administration.
Delays: Every minute counts n=23
In all 23 cases of delay the need was either urgent (11) or emergency (12) and 14/23 (60.9%) patients
were in the ED. Eight patients had delays of more than 10 hours with the longest delay being 36 hours. One patient did not receive the PCC. A large UK-wide study demonstrated notable delays in anticoagulant reversal (Buka, et al., 2025).
Case 15.1: Delayed treatment of haemorrhagic stroke (imputability 1 – possible)
An elderly patient developed neurological deterioration, and the computed tomography (CT) scan demonstrated ICH. PCC was recommended for anticoagulant reversal but was not given before the patient was transferred to a ward. There was communication confusion which resulted in a 5-hour delay in treatment. The patient died and the delayed treatment was considered contributory.
Case 15.2: Head injury and ICH with delayed PCC (imputability 2 – probable)
An elderly patient with atrial fibrillation (AF) fell at home, hit their head and lost consciousness for 5 minutes. They waited 3 hours for a paramedic crew to arrive. A head CT scan showed an acute subdural haematoma. Neurosurgeons advised warfarin reversal with PCC, but this was not achieved for 8 hours. The patient deteriorated neurologically with a subsequent seizure and a massive increase in bleed size. The patient never regained consciousness and passed away.
Learning point
- Many elderly patients are receiving anticoagulants usually due to AF. They have an increased likelihood of falls and are at high risk of ICH. Anticoagulants should be urgently reversed upon identification of ICH.
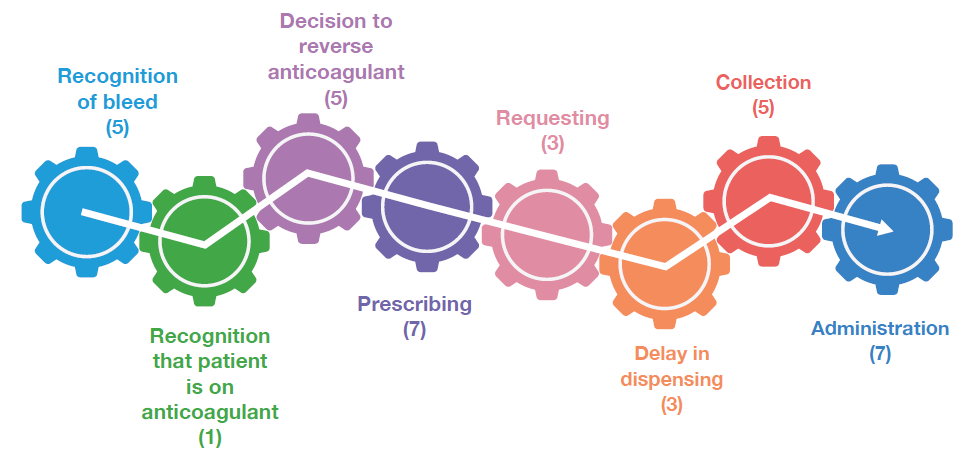
Delays occurred at several points and there were often multiple contributory factors (Figure 15.1).
Figure 15.1: Points of delay in the PCC care pathway, 2025
Communication issues
Communication problems were recorded in 16/39 (41.0%) cases.
Case 15.3: A series of mishaps leading to delayed administration of PCC
A patient on a direct oral anticoagulant (DOAC) was admitted with a haemorrhagic stroke. PCC was prescribed but administered after a 3-hour delay caused by a combination of errors. An incorrectly completed request form sent to the transfusion laboratory had to be rewritten. The form was taken to the transfusion laboratory late because staff were not aware that the request was urgent. The ward staff were not aware that the order was ready. PCC was then delivered by the porter to the wrong ward.
Case 15.4: Lack of communication about PCC storage for emergency use
A patient required emergency above-knee amputation due to necrotising fasciitis. Their INR was 4.9. The haematology consultant advised 2000 international units of PCC and to recheck the INR and give further PCC if INR >1.5. There were multiple telephone calls between the clinical team, the transfusion laboratory and the on-call pharmacist which led to a misunderstanding as to which blood product was required and where it could be found. This resulted in factor IX concentrate (BeneFIX®), being issued from the factor issue refrigerator and administered, instead of PCC. Emergency stocks of PCC were held in the ED but were not listed on the pharmacy ward list on the intranet and could therefore not be located out-of-hours.
Consequently, a poster has been placed on the factor refrigerator in the pathology department advising on PCC location out-of-hours. Theatres have a copy to display in their clinical areas. A quick reference guide is to be developed for on-call pharmacists to delineate the various names which may be used for blood products and where these are kept.
Wrong blood component or blood product n=5
In 5 cases patients failed to receive the correct blood component and/or blood product. A patient with metallic heart valves and gastrointestinal (GI) haemorrhage was prescribed PCC for anticoagulant reversal which is relatively contraindicated because of an increased risk of thrombosis (Uncu, et al., 2024). The balance of risks for the individual patient should be considered.
Three other patients received FFP inappropriately. In 1 case, a patient with a rectal bleed and receiving a DOAC (direct oral anticoagulant) received FFP in addition to unnecessary PCC; a patient with a lower GI bleed on warfarin (non-major haemorrhage) with a history of heart failure was given FFP instead of PCC. A patient had Octaplas® ordered instead of Octaplex®, the error being identified by the transfusion laboratory who questioned the indication for plasma. In the final case, a factor IX analogue was mistakenly ordered instead of PCC (see Case 15.4).
Learning points
- PCC is the reversal agent of choice for warfarin and DOAC (other than idarucizumab specifically for dabigatran).
- Use of trade names and inadequate verbal communication increase the risk of incorrect blood products being administered.
Near miss PCC n=1
PCC was ordered for a patient and sent to the ward. The patient was subsequently put on an end-of-life pathway. The PCC was stored in the ward refrigerator and forgotten for several weeks.
Conclusion
Most reports were submitted were due to delays in provision and administration of PCC, particularly in patients with ICH. Clear communication using non-trade names may avoid confusion and reduce errors resulting in incorrect products being given. Easy access to protocols including clear stock locations, and fixed initial dosing of PCC facilitate timely decision-making, thus helping to reduce errors and delays. The 2023 Annual SHOT Report included a review of evidence for fixed dose PCC in the emergency setting (Narayan, et al., 2024). Systematic reviews have demonstrated benefits: dose reduction, more rapid administration, better haemostasis with reduced mortality and fewer thromboembolic events (Alwakeal, et al., 2024; Homssi, et al., 2025; Schrader, et al., 2026). This year’s reports of delay are consistent with the large UK-wide study mentioned above (Buka, et al., 2025). This study also showed an increased risk of thrombosis associated with the anticoagulant reversal agent Andexanet alpha. At initiation of anticoagulant therapy patients should be counselled about risks of major bleeding, particularly ICH. Elderly patients and their carers should be reminded of this annually, as this could shorten time to presentation for ICH.
Recommended resources
CAS Alert – Preventing transfusion delays in bleeding and critically anaemic patients
SHOT Bite No. 16: Errors with Prothrombin Complex Concentrate