Authors: Caryn Hughes and Debbi Poles
This overview page covers all NM cases – including 992 wrong blood in tube (WBIT), and 378 reports in other NM categories.
Link to PDF chapterKey SHOT messages
Key findings
- NM events continue to be the largest category reported to SHOT despite a slight decrease from 2024. Clinical NM events, including WBIT, accounted for 1213/1370 (88.5%) of NM reports.
- A notable reduction (>45%) of NM events in the right blood right patient (RBRP) and anti-D immunoglobulin (Ig) administration errors categories.
- Component selection and labelling errors were the most common reasons for laboratory NM events.
- Clerical errors at emergency department (ED) registration and corridor care resulted in WBIT events.
- Mix-ups between maternal and cord samples continue to be reported year-on-year.
Gaps identified
- WBIT is most commonly attributed to patients not being identified at phlebotomy and samples being labelled away from the patients’ side.
- Patients identified by bedspace or patients with similar names at the time of the event contributed to WBIT reported from wards.
- Key contributory factors included communication failures, gaps in staff knowledge or skills and workload–staffing mismatch.
Good practice
- Implementation of the confirmatory sample policy allowed detection of WBIT including events that occurred years earlier.
- Almost half of NM events were detected during pre-administration checks.
- A human-factors approach was used in more than 80% of incident investigations, marking an increase compared with 2024.
- Clinical teams taking prompt action once the error was identified including informing the transfusion laboratory.
- Collaboration between different laboratory specialties when discrepant results were detected leading to identification of WBIT.
Next steps
- A structured system for reporting, investigating, and analysing NM events helps identify causes of errors and contributory factors before patient harm occurs.
- NM events offer valuable insights that can inform improvements to processes, systems, and policies, ultimately strengthening transfusion safety.
- Ensure adherence to policies and processes for patient identification and sample labelling.
- Ensure that all staff understand the risks associated with incorrect patient identification.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
NM definition
A ‘near miss’ event refers to any error which if undetected, could result in the determination of
a wrong blood group or transfusion of an incorrect component, but was recognised before the
transfusion took place.
For a more detailed definition see https://www.shotuk.org/reporting/incident/definitions/
Introduction
As in previous years, NM events in 2025 accounted for the largest overall category of cases reported
to SHOT, 1370/4046 (33.9%). Although there was a small decrease in the total number of NM events
compared to 2024 (n=1408), this was still the second highest number of NM events reported since
2019 (Figure 16.1).
The SHOT Transfusion Safety Standards require organisations to report, record, trend and learn from
transfusion‑related near misses, using this intelligence to drive system‑level improvements, strengthen safety controls and prevent patient harm within a just and learning safety culture.
Figure 16.1: A decade of NM (other) and WBIT reports (2016-2025)
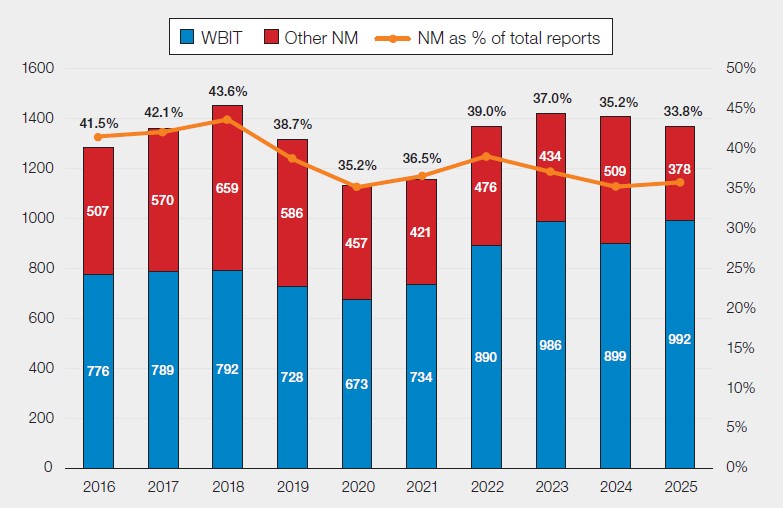
The largest category of NM analysed by SHOT in 2025 was WBIT (n=992), which increased from 899
in 2024 (Figure 16.1). WBIT can lead to ABO-incompatible (ABOi) transfusions which can be fatal and
are covered in a separate chapter (Chapter 16a, Near Miss – Wrong Blood in Tube (WBIT)). Conversely,
NM events in certain other categories showed a decrease of over 45% compared to 2024; RBRP, 125
in 2024 to 65 in 2025 (decrease of 48.0%); anti-D Ig administration errors, 40 in 2024 to 19 in 2025
(decrease of 52.5%).
Table 16.1: Number of NM by SHOT category reported in 2025
| SHOT category | Number of cases in 2025 | Discussed in chapter |
|---|---|---|
| Wrong blood in tube (WBIT) | 992 | Chapter 16a |
| Handling and storage errors (HSE) | 129 | Chapter 11 |
| Incorrect blood component transfused-wrong component transfused (IBCT-WCT) | 105 | Chapter 10 |
| Right blood right patient (RBRP) | 65 | Chapter 17 |
| IBCT-specific requirements not met (SRNM) | 52 | Chapter 10 |
| Anti-D immunoglobulin (Ig) administration errors | 19 | Chapter 9 |
| Avoidable transfusion | 6 | Chapter 13 |
| Delayed transfusion | 1 | Chapter 12 |
| Incidents related to prothrombin complex concentrates (PCC) | 1 | Chapter 15 |
| Total | 1370 |
NM events are discussed in each relevant chapter of the 2025 Annual SHOT Report (Table 16.1).
Most common NM events in laboratory and clinical settings (excluding WBIT)
In 2025, a total of 157 NM events were attributed to laboratory errors and 221 to clinical errors. The
most frequently reported laboratory error categories were RBRP, 44/157 (28.0%), IBCT‑SRNM, 41/157
(26.1%), and IBCT‑WCT, 37/157 (23.6%). Within RBRP, the predominant errors were labelling errors,
32/44 (72.7%) and sample receipt and registration errors, 10/44 (22.7%). For IBCT‑SRNM, the most
common error involved failure to provide irradiated blood components when required, 22/41 (53.7%). In IBCT‑WCT, primary errors were evenly split between provision of an incorrect blood group, 17/37 (46.0%) and issuing a blood component for the wrong patient, 17/37 (46.0%). ABOi transfusions could have taken place in 3 of these cases.
Clinical errors were most reported under HSE, 105/221 (47.5%) and IBCT‑WCT, 68/221 (30.8%). The
majority of HSE errors were related to cold chain failures, 99/105 (94.3%). IBCT-WCT were mostly due
to errors during blood component collection, or prior to administration to the wrong patient, 67/68
(98.5%). Detection of these errors prevented 17 ABOi transfusions.
Case 16.1: ABOi transfusion prevented by pre-administration checks
A porter collected a unit of red cells from the blood issue refrigerator for patient 1 (group A D-positive) who had the same first name and surname as patient 2 (group B D-negative) without performing robust safety checks. The porter was distracted by a colleague, and there was also a backlog of tasks due to a long-running major haemorrhage call on the previous shift. The unit of red cells was received in the clinical area and when the nursing staff were completing their pre-administration checks at the patient’s bedside, they noticed that the date of birth and unique patient identification number on the blood component did not match the details on the patient identification band. They contacted the blood transfusion laboratory and arranged for the unit of red cells to be returned.
This case highlights the importance of completing the final pre-transfusion checks at the patient’s side which prevented the potentially serious consequences of receiving an ABOi blood component.
Contributory factors in near miss errors
A total of 309/378 (81.7%) non-WBIT reports used a human‑factors‑based approach during investigation. Communication failures were identified as contributory factors in 132 cases. In 122 NM events, a mismatch between workload and staffing levels at the time of the event was reported, while 120 cases cited gaps in staff knowledge or skills as significant contributing factors.
Conclusion
NM events remain the most frequently reported category to SHOT, with clinical WBIT continuing to feature prominently. It is important to recognise and monitor trends in NM events. While some reduction in NM RBRP and NM anti-D Ig events have been observed, this must translate into a genuine reduction in harm events. NM data should be used to drive optimal learning and targeted improvements in order to strengthen systems and enhance overall safety. Key contributory factors for the reported NM included deficiencies in communication, gaps in staff knowledge, and pressures related to staffing levels. The detection of errors during pre-administration checks highlights the effectiveness of existing safety barriers, the findings reinforce the need for stronger processes, enhanced staff training, and greater system resilience.
Recommended resources
SHOT Transfusion Safety Standards
SHOT Bite No. 17: Learning from Near Misses (NM)
Near Miss (NM) Cumulative Data page
