Authors: Vera Rosa, Paula Bolton-Maggs and April Molloy
Link to PDF chapter Link to supplementary informationGlossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
WBIT definition
Blood is taken from the wrong patient and is labelled with the intended patient’s details.
Blood is taken from the intended patient but labelled with another patient’s details.
For a more detailed definition see https://www.shotuk.org/reporting/incident/definitions/
Introduction
WBIT reports continue to represent the largest proportion of near miss (NM) events reported to SHOT,
992/1370 (72.4%). This is the highest number of WBIT reported to SHOT in a year. In 932/992 (94.0%)
cases the process for sample labelling was provided; in 804/932 (86.3%) the sample was handwritten
and in 128/932 (13.7%) the sample was labelled using an electronic system.
Causes of error
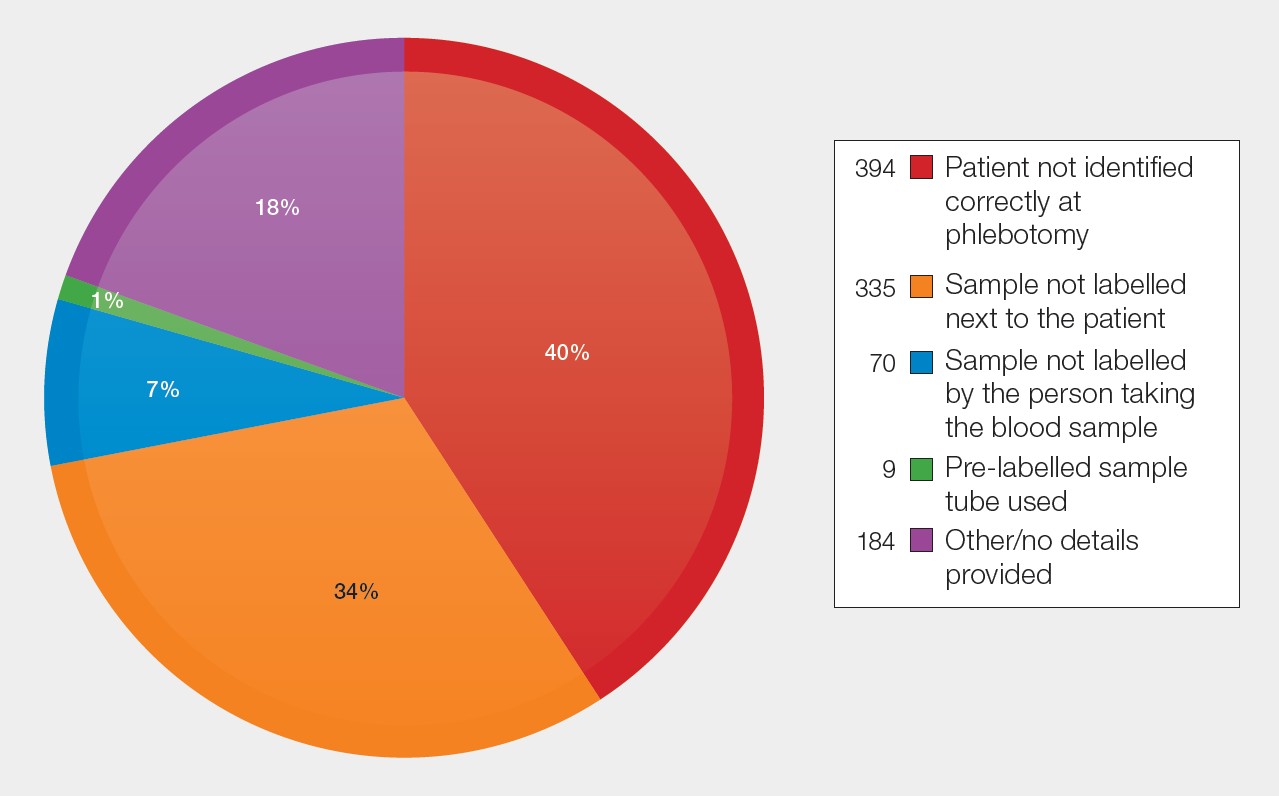
As in previous years, the two main causes for WBIT continue to be
- Failure to identify the patient correctly at phlebotomy, 394/992 (39.7%)
- Labelling the sample away from the patient, 335/992 (33.8%) (Figure 16a.1)
In 219/729 (30.0%) cases both errors occurred together with or without additional causes contributing to the same event.
Figure 16a.1: Primary causes of WBIT in 2025 (n=992)
Point of detection
In 165/992 (16.6%) cases the clinical team recognised the error and contacted the laboratory. In 4 cases, haematology and biochemistry were notified, but not blood transfusion. Recognition and communication occurred at various sample process stages. In 58/992 (5.9%), the historical group and screen samples were identified as WBIT; these were often detected by the confirmatory sample requirement highlighting its importance for transfusion safety.
Figure 16a.2: Point in the process where the error was detected in WBIT reported in 2025 (n=992)
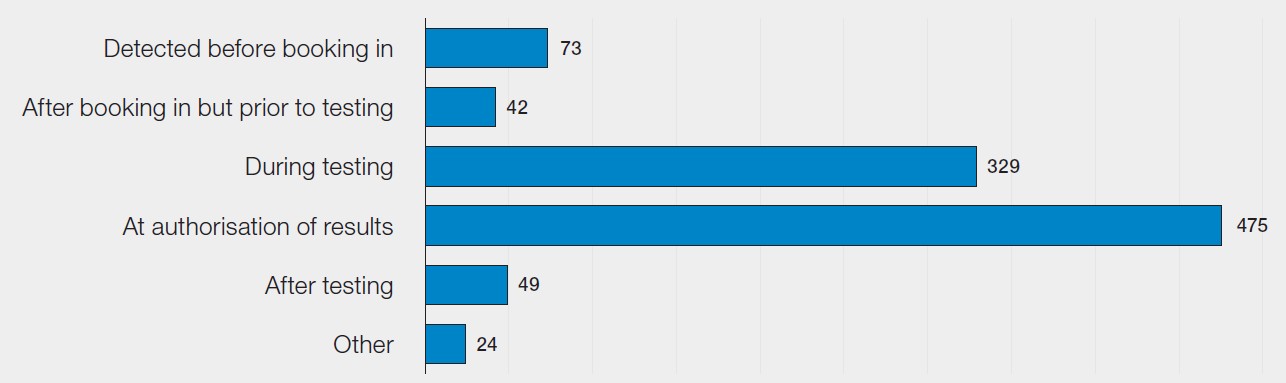
The WBIT identified after testing being completed (49/992) were often detected when clinicians were
reviewing the patient results. These cases were not detected by the laboratory because either the blood group of the WBIT was the same as the intended patient or the incorrectly taken sample was the first record of the patient in the laboratory.
Case 16a.1: Discrepant full blood count results identify a WBIT
Samples were taken from a patient for haematology, biochemistry and blood transfusion laboratories. Upon testing, the full blood count (FBC) showed pancytopenia which was discrepant with the patient’s previous results. A repeat FBC confirmed that the first sample was a WBIT. Biochemistry and transfusion samples taken at the same time were rejected. Following investigation, it was identified that at the time of the event there was an unusually high number of staff on annual leave and sick leave and many requests for phlebotomy. In this case the request form had been labelled with the incorrect patient’s bed number which resulted in the incorrect patient being bled.
Case 16a.1 highlights the importance of collaboration and timely communication between different pathology disciplines when discrepant results are identified in one area. It also shows the risks of identifying patients only by bedspace rather than full patient details.
ABO-incompatibility (ABOi)
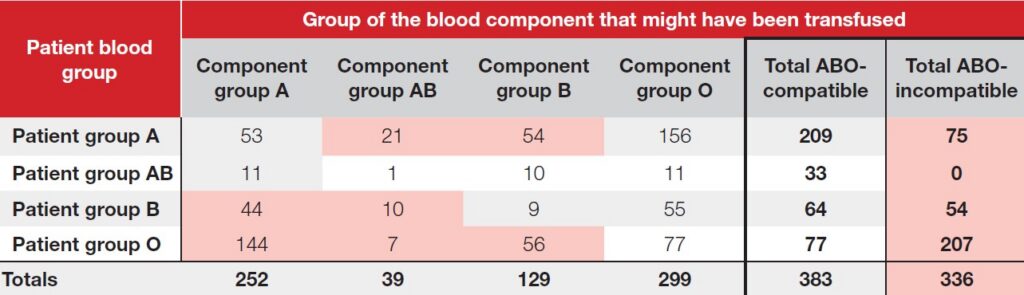
Blood groups of the intended patient and of the WBIT sample were provided in 719/992 (72.5%) reports. Table 16a.1 shows the patient blood groups, and the blood group of the red cell units that would have been issued/administered based on the WBIT result. In 336/719 (46.7%) the intended patient could have received an ABOi red cell transfusion with potential risk for serious harm or death.
Table 16a.1: Potential for ABOi red cell transfusion as a result of WBIT in 2025
Errors in non-maternity cases n=593
Non-maternity cases represented more than half of the WBIT, 593/992 (59.8%). These cases involved
490 routine samples and 53 urgent requests with potential to cause delays in transfusion, suboptimal
care and/or avoidable use of emergency blood group O units. It is notable that 168/593 (28.3%) of cases were from the emergency department (ED).
Case 16a.2: Multiple staff involved in sample taking and labelling to avoid delays
A group and screen (G&S) sample was taken by a resident doctor and handed over to a locum doctor for labelling. The locum doctor did not have access to the printer, so the sample was passed to the nurse. The nurse felt reluctant to label a sample that they had not taken but did not feel confident to challenge the request. Additionally, the nurse was aware that delays in sending the sample might lead to surgery cancellation. The WBIT was identified in the laboratory when the blood group did not match the patient’s previous record.
To minimise the risk of transfusion errors, the same individual who takes the blood sample should label it immediately at the patient’s side. The sampling and labelling process must not be interrupted, as distractions or handovers increase the risk of misidentification and serious patient safety incidents (Robinson, et al., 2018).
Errors in maternity cases n=399
In 2025, 399/992 (40.2%) reports were related to maternity, 339 were routine cases while 33 were
emergency. More than 80% of the urgent samples (27/33) were from obstetrics. The two most common locations were obstetrics, 214/399 (53.6%) and antenatal clinics, 100/399 (25.1%).
Errors reported with maternal and neonatal samples included:
- Mother and cord mix-ups (n=48); 2 identified in a retrospective audit and 1 through high-throughput non-invasive prenatal testing for fetal RHD genotype (cell-free fetal deoxyribonucleic acid (cffDNA)) discrepancy
- Confusion in sampling twins including cord samples (n=5)
- Cord samples taken from the wrong placenta (n=4); 1 historical WBIT from 2009
- Cord samples mislabelled (n=2); 1 swap between mother and baby (not cord) samples
- Neonatal samples taken from the wrong baby (n=3)
Case 16a.3: Assumed clerical error and incorrect patient record amended
A midwife registered a pregnant woman new to the healthcare organisation under a hospital number belonging to a different patient. Both individuals had the same forename, surname and year of birth. When the midwife confirmed the details with the woman and identified the discrepant date of birth, the midwife assumed that a clerical error had been made at registration and amended the details and previous records on the system. When the G&S sample was tested in the laboratory the WBIT was identified as the blood group did not match previous record. Both women were contacted, and the error rectified.

Human factors and systemic gaps identified in the 2025 WBIT reports
Table 16a.2 shows the most commonly reported human factors to SHOT via the Human Factors
Investigation Tool (HFIT), including local working conditions, environment, workload, organisational and staffing levels, communication, and situational factors.
Table 15a.2: Human factors that contributed to the WBIT cases in 2025
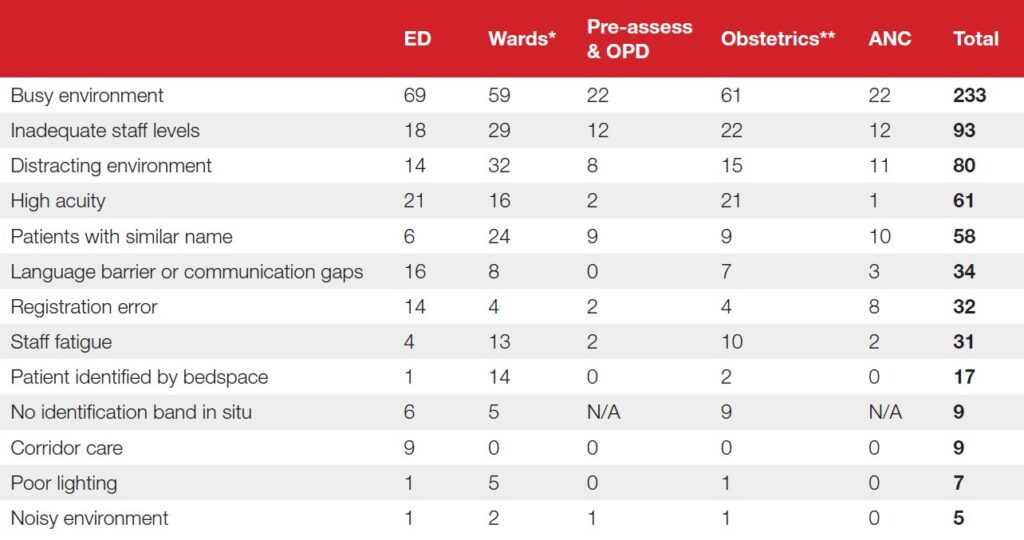
*Wards also include cases from high dependency and intensive care units
**Obstetrics also include cases from neonatal and paediatric settings
Common to all settings
A busy environment during blood sampling was the most common contributory factor across all settings. Distractions, high acuity, and inadequate staffing levels increased pressure on staff. Staff fatigue was also noted. Staff fatigue is commonly a hidden safety risk that should be escalated and recognised. The impact of fatigue on safety has been highlighted by the Health Services Safety Investigation Body (HSSIB, 2025b).
Emergency department
In 14 cases, while the ED was documented as the location of the error, investigation showed that the
errors occurred earlier in the process, reinforcing the importance of analysing whole‑system failures rather than focusing on the point of detection. In some of these, the incorrect patient identification occurred before the patient arrived at hospital (e.g., in the ambulance). In 9 cases patients were receiving care in corridors. These reports reflect the risks for patient safety highlighted by different organisations (RCEM, 2025; RCP, 2025; Iacobucci, 2026).
Learning points
- Accurate and complete patient identification is essential: patients must not be identified by bedspace.
- Following identification, labelling the sample next to the patient must be performed as one continuous uninterrupted process.
- Staff fatigue must be recognised, escalated and managed appropriately by the organisation to ensure staff and patient safety.
- Corridor care imposes a safety risk for patients leading to workarounds and suboptimal care.
Conclusion
Failure to identify patients at phlebotomy and labelling samples away from the patient remain the most common and often co-occurring errors. These are frequently linked to distraction, high patient acuity, busy working environments, and staff fatigue. To reduce risk, samples should be taken and labelled in one uninterrupted process at the patient’s side following positive patient identification.
Recommended resources
Meet the experts webinar: Near Miss Reporting & Wrong Blood in Tube (WBIT)
Pre-transfusion Blood Sampling Process
Chapter 15a – Near Miss – Wrong Blood in Tube (WBIT) – Supplementary Data 2024