Authors: Tracey Tomlinson, Anicee Danaee, Victoria Tuckley and Nicola Swarbrick
Link to PDF chapter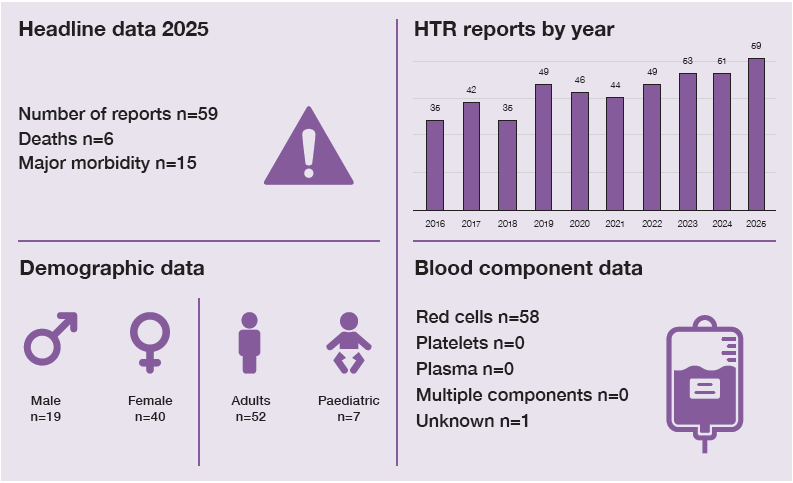
Key SHOT messages
Key findings
- The number of HTR reported is showing an upward trend over the past 10 years.
- Reporting of hyperhaemolysis (HH) is increasing with most cases occurring in patients with sickle cell disorder (SCD).
Gaps identified
- There has been a decline in the availability of pre- and post-haematology and chemistry results making confirmation of HTR difficult.
- Lack of historical antibody information increases the risk of HTR.
Good practice
- There has been an increasing trend in reporting of HH cases.
- SHOT data has helped improve the data available on treatments used to manage HH.
Next steps
- Promote education and awareness to improve HTR diagnosis and distinction from disease complications, including escalation pathways and post-transfusion testing.
- Ensure information on previous antibodies is included in patient records and shared-care
documentation, and is accessible to all relevant staff. - Encourage timely, complete SHOT reporting to improve learning and guide future safety initiatives.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
HTR definition
Acute haemolytic transfusion reactions (AHTR) are defined as fever and other symptoms/signs of haemolysis within 24 hours of transfusion. Delayed haemolytic transfusion reactions (DHTR) are defined as fever and other symptoms/signs of haemolysis more than 24 hours after transfusion. Hyperhaemolysis is characterised by more severe haemolysis than DHTR with haemolysis affecting the transfused red cells and the patient’s own red cells, causing a haemoglobin drop to below post-transfusion levels.
For a more detailed definition see https://www.shotuk.org/reporting/incident/definitions/
Introduction
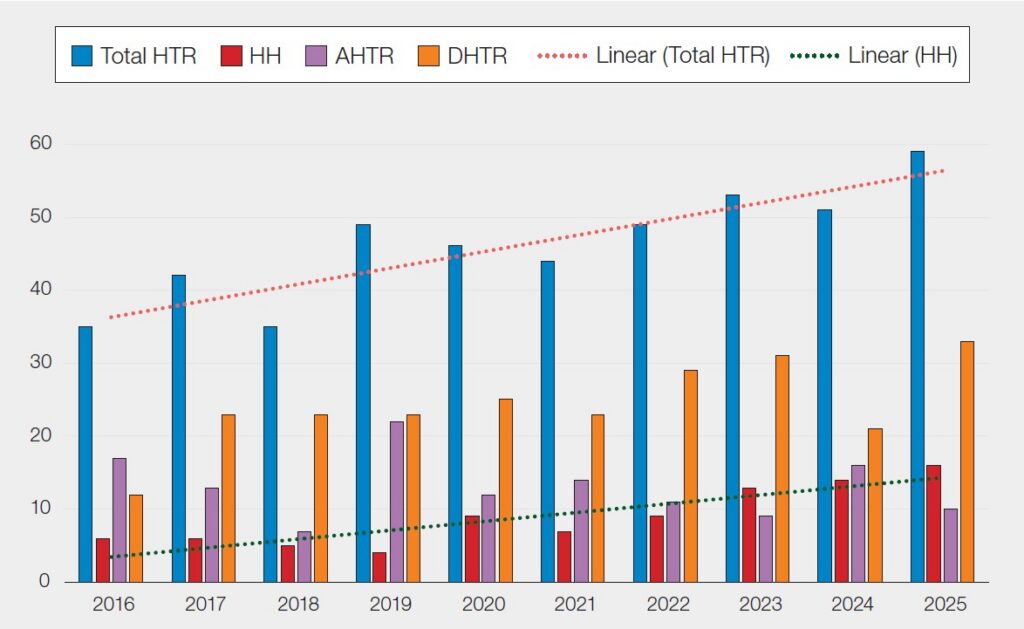
In 2025 there were 59 HTR reported which is an increase from 2024 (n=51). The data demonstrates an
upward trend in HTR reported to SHOT and a corresponding increase in reports of HH (Figure 22.1).
Using the HTR definitions described above, the cases analysed in 2025 were subdivided into 10 AHTR,
33 DHTR and 16 HH cases.
Figure 22.1: Total number of haemolytic transfusion reactions (HTR) reported by year (2016-2025)
The reaction occurred following red cell transfusion in 58 of the 59 cases. The component type was
not specified in 1 case; however, from the transfusion details provided this was also most likely due to
red cell transfusion.
Deaths related to transfusion n=6
HTR were implicated in the deaths of 6 patients: 1 of these was imputability 3 (definitely related to the
transfusion reaction); 2 were imputability 2 (probably related); and 3 were imputability 1 (possibly related). This included HH reactions in 5 patients who were being treated for SCD and a 6th case occurred in a patient with complex red cell phenotype matching requirements. This case is still under investigation and learning will be shared once this is completed.
Major morbidity n=15
Major morbidity was reported in 15 cases. The majority of these occurred in patients who experienced HH (n=11), corresponding to the SHOT definition that all cases of HH are considered as a major morbidity. Major morbidity was most frequently reported in patients with SCD and was associated with HH in 9 patients and DHTR in 2 patients. There were also 2 cases in patients with thalassaemia (1 HH and 1 AHTR), 1 cancer patient (DHTR) and 1 Diamond-Blackfan anaemia patient (HH).
Patient demographics
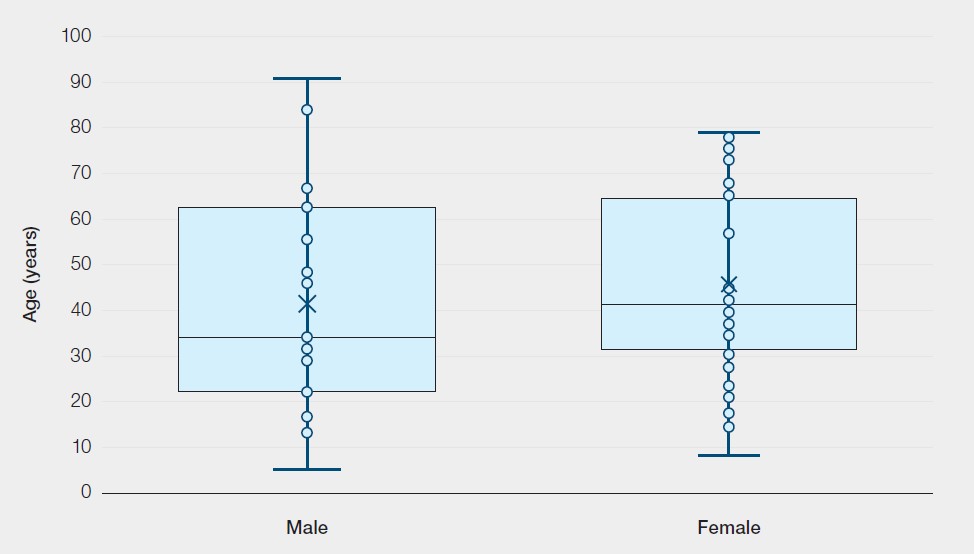
The age range was 5 to 91, with a median age of 41. HTR were reported in 7 paediatric patients. Age
range and gender are shown in Figure 22.2. More than half, 40/59 (67.8%), of the reactions occurred
in female patients.
Figure 22.2: Age range in males and females experiencing HTR in 2025 (n=59)
Acute haemolytic transfusion reactions n=10
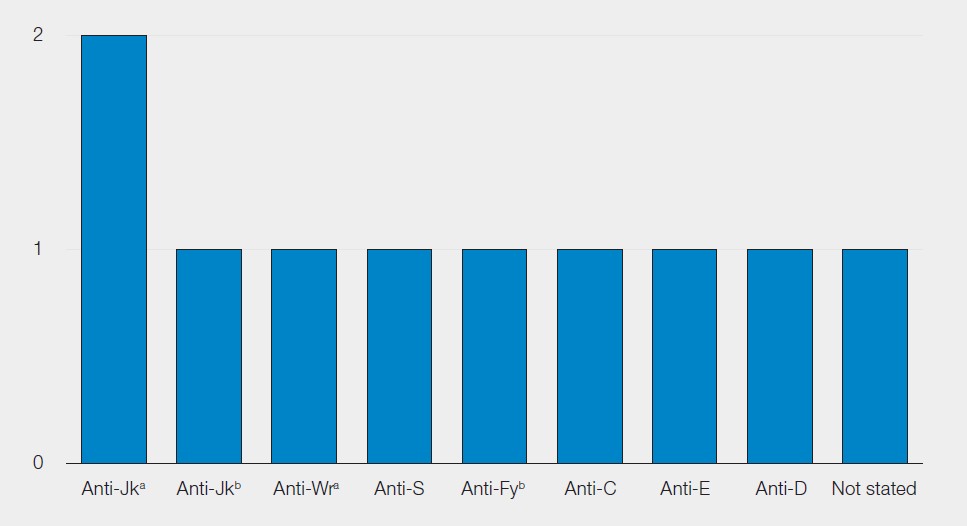
Two cases involved the transfusion of ABO-matched red cells issued in an emergency situation prior to the completion of pre-transfusion testing. It is important that lifesaving transfusion is not withheld due to a history of alloantibodies. In urgent clinical situations where suitable antigen-negative blood is not available it may be necessary to transfuse blood which is positive for a confirmed antibody (SHOT Bite No.8).
One AHTR was due to the presence of anti-Wra, an antibody directed to a low prevalence antigen which was not present on the screening cells used. There was also 1 case reported in which no apparent red cell antibodies were detected.
In addition to the 10 AHTR included in this chapter, there were 4 acute reactions due to ABO-incompatible red cell transfusions; 3 led to major morbidity, and 1 was a mild reaction. These are all included and discussed in Chapter 10, Incorrect Blood Component Transfused (IBCT).
Figure 22.3: Antibodies implicated in AHTR in 2025
Delayed haemolytic transfusion reactions n=33
DHTR remains the most common HTR reported to SHOT accounting for over half of the cases (33/59).
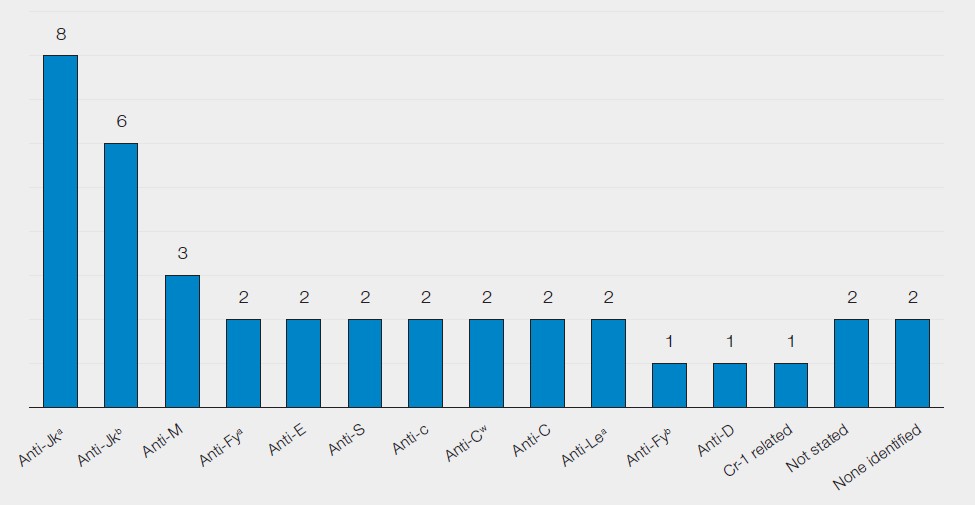
In the majority of DHTR (26/33) the patient did not suffer serious harm, however there were 3 cases with major morbidity and 1 patient death related to the transfusion reaction. Like previous years, many of the DHTR reported were due to the presence of historical red cell antibodies that were not detected during the pre-transfusion testing for the implicated transfusion. This is often due to the antibodies dropping below detectable levels. This risk can be mitigated if information on previously detected antibodies are included in patient records including shared-care documentation. Antibodies to the Kidd (Jk) blood group system remain the most frequently antibody specificity implicated in DHTR.
Figure 22.4: Antibodies implicated in DHTR in 2025
Hyperhaemolysis reactions n=16
While the number of HH cases reported was higher than in previous years, HH may still be under-reported as it can be difficult to diagnose, with symptoms showing many similarities to DHTR and vaso-occlusive crisis (Adkins, et al., 2020). The increasing trend in reports may represent timely identification and recognition of HH as knowledge improves.
The majority of HH cases continue to be reported in patients with SCD (14/16). Of the 2 remaining
cases, 1 occurred in a patient with thalassaemia and 1 in a patient with Diamond-Blackfan anaemia.
HH can be divided into acute and delayed HH. Acute HH occurs within 7 days of transfusion, and
the DAT is usually negative. Delayed HH occurs more than 7 days post transfusion and the DAT is
often positive. In contrast to a classical DHTR, in delayed HH both patient and transfused red cells are
haemolysed (Danaee, et al., 2015). In 2025, 9 cases were categorised as acute HH and 7 as delayed.
Treatment in hyperhaemolysis
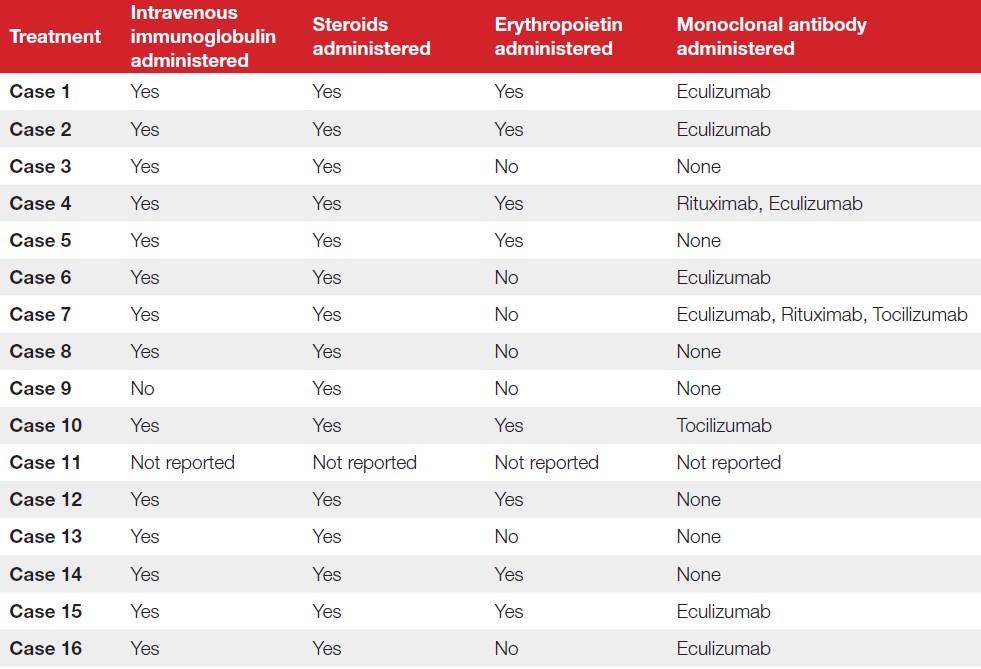
SHOT has been collecting information on HH treatment modalities since 2020 with the aim to provide a better understanding of practice nationally and improve and share knowledge. Eculizumab is licensed to treat ongoing brisk haemolysis (NHSE, 2020a) and was reported as being used in 7/16 cases. SHOT data demonstrates a move towards using of a combination of different treatments with 5/16 (31.3%) receiving intravenous immunoglobulin (IVIg), steroids and erythropoietin (EPO) in addition to monoclonal antibody therapy. A summary of the pharmacological treatment methods used in each of the 2025 cases is provided in Table 22.1.
Table 22.1: Pharmacological treatments used to manage cases of HH reported to SHOT in 2025 (n=16)
Learning point
- Early recognition of HH, particularly in patients with SCD, with prompt escalation to haematology and transfusion specialists can improve clinical decision-making and enhance patient outcomes.
Diagnosing HTR
The identification of HTR remains challenging, as many of the classical signs and symptoms are common to other clinical conditions. It is therefore essential that both clinical observations and laboratory results are closely monitored and reviewed to obtain a comprehensive picture of the patient’s condition. Failure to correctly identify HTR can delay appropriate management and the implementation of measures to ensure the safety of future transfusions.
Conversely, incorrectly diagnosing HTR can result in other underlying issues being overlooked and may cause unnecessary anxiety for both patients and clinical staff. The British Society for Haematology (BSH) guideline for administration of blood components emphasises the importance of close monitoring of all transfusion recipients, including repeat post-transfusion haematology and biochemistry testing (Robinson, et al., 2018). However, SHOT is observing a concerning increase in reports where the post-transfusion testing has not been completed or is not available, which represents a missed opportunity for early detection of HTR and intervention. Consistent clinical surveillance, appropriate laboratory investigation, and prompt reporting are essential to improve patient outcomes and support national learning.
Learning points
- Maintain strict post-transfusion monitoring, including repeat haematology and biochemical testing, especially following emergency blood issue.
- Promote multidisciplinary education and awareness to support accurate diagnosis of HTR and differentiation from underlying disease complications.
Mitigating against HTR
Each year SHOT receives reports of patients with a history of red cell antibodies experiencing HTR following the transfusion of antigen-positive red cells. HTR can be very distressing to both patients and the treating clinical teams. Whilst it is impossible to prevent all HTR, the risk can be mitigated by robust pre-transfusion procedures which include checking for a history of red cell antibodies. These cases are most often associated with patients receiving care in multiple hospitals. In 2025, there were 6 such cases reported. One involved the planned transfer of a patient with a known anti-Jka, but the transfer handover did not include this information. In each of the other cases a record of the antibody was available on Specialist Services Integrated Clinical Environment (Sp-ICE), however this was only accessed after the transfusion occurred. An incomplete antibody history remains a major contributory factor to HTR and urgent action is required to address this.
Learning points
- Strengthen management of historical antibodies through robust record-keeping, shared-care systems, and consistent review of antibody histories prior to transfusion.
- Ensure reliable access to complete red cell antibody histories by strengthening inter-hospital communication, transfer handover processes and routine checks of shared laboratory systems prior to transfusion to prevent avoidable HTR.
Conclusion
Reports of HTR to SHOT in 2025 demonstrate a statistically significant upward trend compared with
the previous 10 years (linear regression trend test; t‑test for non‑zero slope, p=0.00063), with DHTR
remaining the most frequently reported subtype (Figure 22.1). This may be partly explained by the increase in reported HH cases, which accounted for the majority of transfusion‑related deaths and major morbidity, predominantly among patients with SCD. Importantly, greater recognition and reporting of HH should be considered a positive development. These findings highlight HH as a critical patient safety issue requiring heightened clinical awareness, early recognition, and timely access to specialist advice.
Recommended resources
Haemolytic Transfusion Reactions (HTR) Cumulative Data
SHOT Bite No. 15: Hyperhaemolysis
SHOT Bite No. 31: The role of Sp-ICE in preventing Haemolytic Transfusion Reactions (HTR)