Authors: Caryn Hughes and Shruthi Narayan
Link to PDF chapter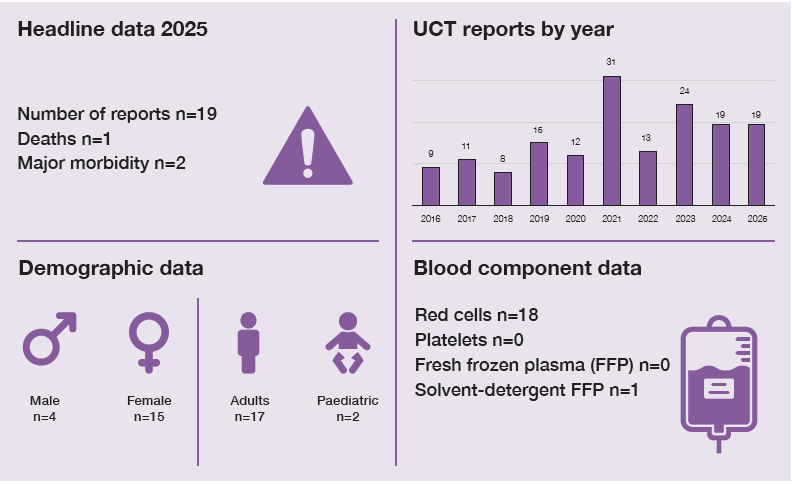
Key SHOT messages
Key findings
- There were fewer paediatric cases reported compared to 2024.
- Incomplete reporting details (e.g. patient observations, laboratory test results etc.) limit the reliability of analysis and conclusions.
Gaps identified
- Inconsistencies in verifying infusion pump settings against the prescribed transfusion rate may lead to rapid administration of blood components and increase the risk of patient complications.
- Limited clinical and laboratory information makes accurate assessment of reports more difficult.
- Learning from these events is not always evident from reports.
Good practice
- Prompt referral, thorough assessment, and timely intervention resulted in the diagnosis of a rare complication of transfusion.
Next step
- Reporters are encouraged to provide complete details and continue submitting cases involving atypical transfusion reactions. Comprehensive reporting improves understanding of these rare complications, helps identify contributing risk factors, and supports the development of effective risk‑reduction strategies.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
UCT definition
Pathological reaction or adverse effect in temporal association with transfusion which cannot be attributed to already defined side effects and with no risk factor other than transfusion and do not fit under any of the other reportable categories, including cases of transfusion-associated hyperkalaemia.
For a more detailed definition see https://www.shotuk.org/reporting/incident/definitions/
Introduction
This category covers unusual transfusion reactions that cannot be classified elsewhere in the definitions to ensure all relevant learning is captured. Many cases involve patients with multiple co-morbidities, which may contribute to the complications. Systematic documentation and review of these cases support continuous learning, improve understanding of transfusion-related risks, and promote patient safety through targeted risk-reduction measures.
Deaths related to transfusion n=1
There was 1 death reported in this category assessed as possibly related to the transfusion (imputability 1).
Case 23.1: Acutely unwell patient with severe renal impairment and hyperkalaemia (imputability 1 – possible)
A patient with microcytic hypochromic anaemia who presented with pallor and a raised respiratory rate received a red cell transfusion in the emergency department (ED). Approximately 10 minutes after commencement, the patient deteriorated, experienced cardiac arrest, and died. Subsequent review revealed the transfusion was initiated before the availability of blood test results showing severe kidney impairment and hyperkalaemia. Post-transfusion investigations were limited due to the unused blood component being discarded and incomplete documentation which was attributed to the clinical workload exceeding available staffing. The pathologist recorded the cause of death as cardiac arrest secondary to hyperkalaemia, blood transfusion, severe anaemia, and acute kidney injury.
Although there was a temporal association between the transfusion and the death of this severely unwell patient, it is difficult to attribute causality. Multiple factors are likely to have contributed. This case highlights the challenges of providing transfusion support in critically unwell patients and underscores the importance of careful clinical assessment, thorough review of investigations, and timely, accurate documentation.
Major morbidity n=2
Case 23.2: Ocular ischaemic complications following rapid red cell transfusion
A patient with a relapsed seminoma receiving chemotherapy had a red cell transfusion over 30 minutes instead of the prescribed 2 hours due to incorrectly set infusion pump parameters. Post transfusion, the patient was subsequently discharged home and 48 hours later presented in the ED with visual changes. There was no evidence of any visual impairment at the time of or prior to the transfusion. Ophthalmology review noted slow-flow retinopathy, possible right central retinal artery occlusion at the time of transfusion, and bilateral ocular ischaemic syndrome.
Retinal artery occlusion immediately after a red cell transfusion has been documented but is extremely rare. In 90% of cases, non-arteritis causes include cardiovascular risk factors, thromboembolism, metabolic or infectious disorders, haematologic malignancies, hypercoagulability, and rarely, blood transfusion reactions (Zapata, et al., 2021).
Multiple factors may have contributed to this event, including the patient’s underlying relapsed cancer, potentially thrombogenic chemotherapy, and the rapid red‑cell transfusion. It is unclear whether any additional pro‑thrombotic factors were present. Thrombogenic chemotherapy can increase the risk of retinal or venous occlusion, especially in individuals with pre‑existing vascular risk factors, but limited information about this patient’s specific treatment prevents any firm assessment of increased risk or a definite link to ocular ischaemic syndrome. Given these uncertainties, the imputability was recorded as likely/probable.
Case 23.3: Cardiac arrest following red cell transfusion in severe anaemia
A haemodynamically stable patient with menorrhagia presented to the ED with a haemoglobin level of 37g/L. The patient received two units of red blood cells but subsequently experienced a cardiac arrest, necessitating admission to the intensive care unit (ICU). A computed tomography pulmonary angiography ruled out a pulmonary embolism, but did detect widespread lung consolidation interlobular septal thickening, dilated left ventricle, soft tissue oedema (suggestive of cardiac dysfunction, possibly high-output state from anaemia). No other cause for the cardiac arrest was identified aside from its temporal association with the transfusion. The patient was stabilised and continued to receive care on the ICU. No further information was available.
The haemodynamic impact of severe chronic anaemia is often overlooked in clinical practice. Severe anaemia can precipitate a high-output cardiac state despite apparent haemodynamic stability, placing patients at significant risk of decompensation (Mehta & Dubrey, 2009). The patient had clear evidence of cardiopulmonary compromise, including consolidation and cardiac failure, indicating multiple ongoing health issues.
Learning points
- Recognising rare yet serious transfusion complications allow for earlier intervention and targeted management.
- Haemodynamic stability does not equate to cardiovascular safety in severe anaemia.
Other cases n=16
Additional cases presented with nonspecific symptoms, including tachycardia, dizziness, vasovagal episodes, seizures, and rashes. Two exchange transfusion cases showed evidence of citrate toxicity, and 1 paediatric patient with beta-thalassaemia major developed generalised leg pain and headache requiring hospitalisation. Imputability in all cases was assessed as possible or likely/probable. These cases are described in more detail in the supplementary information on the SHOT website.
Conclusion
This chapter contains a range of clinical scenarios in which, beyond a temporal association with transfusion, a clear causal link cannot always be established. Nevertheless, careful assessment and consideration of any potentially preventable contributing factors remain essential for improving patient safety. Although transfusion is generally safe, complications can occur and may be difficult to recognise, particularly in patients with complex or evolving clinical conditions. Atypical or rare reactions that occur close to transfusion should be promptly identified, managed, and reported to SHOT. Even when causality is uncertain due to coexisting medical or surgical issues, systematic review of these cases is vital to ensure learning and strengthen future practice.
