Authors: Tali Yawitch, Katy Davison and Su Brailsford
Link to PDF chapter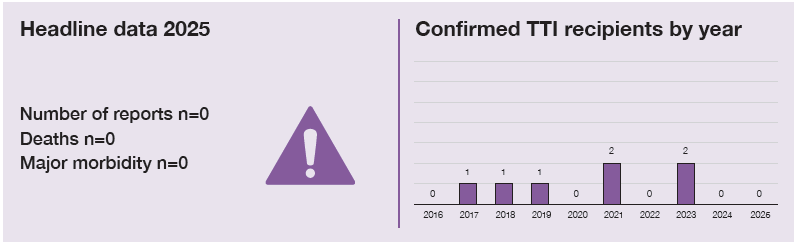
Key SHOT messages
Key findings
- There were no confirmed TTI reported in 2025.
- There were three bacterial near miss cases reported in 2025.
Gap identified
- Current safety measures, although extremely effective, cannot prevent all TTI. Colleagues are encouraged to check for visually abnormal units and remain alert for transfusion reactions.
Good practice
- Visual inspection of blood component packs by vigilant staff at various steps in the transfusion pathway has helped to reduce TTI. Three near miss incidents (Staphylococcus aureus) were detected.
- The United Kingdom (UK) Blood Services store a sample from every blood donation for at least 3 years, allowing testing of these archived samples if a TTI is suspected.
- Use of the Annual SHOT Report data helped to inform policy and prompt necessary changes to improve safety.
- The UK Blood Services continuously monitor infection rates in donors to provide assurance of the blood supply.
Next steps
- Hospitals are encouraged to report suspected TTI to the appropriate UK Blood Service for further investigation when there are no other obvious risks.
- The consultant microbiologists, virologists, and/or other infectious disease experts should be consulted to confirm the diagnosis of a suspected TTI.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
TTI definition
Included as a TTI if, following investigation, the recipient had evidence of infection post
transfusion, there was no evidence of infection prior to transfusion and no evidence of an
alternative source of infection.
AND
Either at least one component received by the infected recipient was donated by a donor who
had evidence of the same infection.
Or at least one component received by the infected recipient was shown to contain the agent of
infection. These may be identified because of infection in the recipient where transfusion is the
suspected source, and a post-transfusion infection reported to the Blood Services.
Alternatively, an infection in a recipient may be identified from lookback investigations which
are initiated when a donation from a repeat donor is identified as having markers of infection.
Archive samples are retrieved for retrospective testing, which may find a previous donation to
also be positive but with markers of infection below the detection level of routine screening. In
this case further work will be carried out to identify recipients.
Note that for the purposes of the European Union legislation, serious adverse reactions (SAR) are defined as any reactions in patients that are ‘life-threatening, disabling or incapacitating, or which result in, or prolongs, hospitalisation or morbidity’. These must be reported to the Medicines and Healthcare products Regulatory Agency (a legal requirement). This includes all confirmed transfusion-transmitted infections.
For a more detailed definition see SHOT Definitions
Introduction
This chapter describes suspected TTI incidents investigated by the UK Blood Services and reported to the UK Health Security Agency (UKHSA) and National Health Service Blood and Transplant (NHSBT) joint Epidemiology Unit’s surveillance scheme in 2025. Additionally, a summary of the lookback investigations in England of newly identified infections in repeat donors is provided. This is to lookback at their previous donation(s) for evidence to exclude transmissions to recipients.
Summary of investigations in 2025
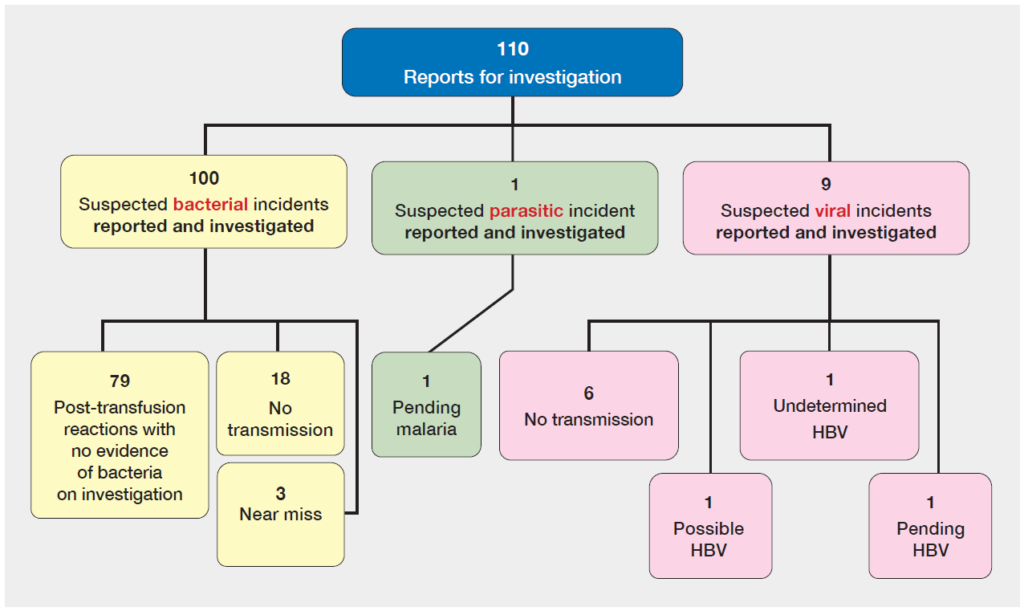
In 2025, the UK Blood Services investigated 100 suspected bacterial incidents and 10 suspected viral
or parasitic incidents (Figure 24.1). No transmissions have been identified; one possible hepatitis B virus (HBV) and one undetermined HBV have been concluded, as well as three bacterial near miss events. Two investigations are pending with investigations still ongoing: one HBV and one malaria.
Figure 24.1: Outcomes of suspected TTI investigated in 2025 and reported to NHSBT/UKHSA
Epidemiology Unit for England, Northern Ireland, Scotland, and Wales
Please note:
- TTI of hepatitis C virus (HCV), hepatitis E virus (HEV), human immunodeficiency virus (HIV) or
human T-cell lymphotropic virus (HTLV) identified either before routine screening or through national lookbacks following the implementation of screening are recorded separately and do not form part of the main Annual SHOT Report numbers. - A confirmed TTI is as per the definition with evidence that the virus/bacterium is indistinguishable
on molecular typing between patient and donor/donation. - A probable TTI is as per the definition, but where molecular typing cannot be conducted to confirm this.
- A possible TTI is as per the definition, but where prior infection or an alternative source could not
be completely excluded. - No transmission is defined as an investigation that concluded the infection in the recipient was NOT caused by transfusion, either as all indicated donors were traced and none of them were shown to be infected; or there was no evidence of infection in the recipient; or they were shown to be infected already prior to transfusion.
- A near miss refers to the detection of an infected blood pack prior to transfusion, identified either
through a visible abnormality or following a donor’s post-donation report of infection. The implicated unit is recalled and tested for infection. For example, bacterial growth identified following culture of a pack returned for investigation. - An undetermined conclusion is when the investigation has been completed as far as possible,
however it is not possible to confirm or refute blood transfusion as cause of infection in recipient.
Deaths and major morbidity related to transfusion n=0
There were no reported deaths or major morbidity cases associated with TTI in 2025.
Near miss n=3
There were three near miss events reported in 2025.
Bacterial TTI reports in 2025
Since 2011, all four UK Blood Services have used the BacT/ALERT system for bacterial screening of
platelets which has been successful in reducing the risk of bacterial TTI, together with diversion and
arm cleansing (McDonald, et al., 2017). In 2025, a newer BactT/Alert Virtuo bacterial screening system
was introduced in some services.
Table 24.1: Bacterial screening of platelets – methods used by the UK Blood Services
| Blood Service | Time of sampling (hour) | Volume sampled (mL) | Apheresis sample | Time at release (hour) | Length of screening |
|---|---|---|---|---|---|
| NHSBT | ≥36 | 2 x 8 | Post-split | 6 | Day 7 |
| NIBTS | ≥36 | 16 | Pre-split | 6 | Day 7 |
| SNBTS | ≥36 | 2 x 8 | Pre-split | 6 | Day 7 |
| WBS | ≥36 | 2 x 8 | Post-split | 12 | Day 7 |
In 2025, no reported suspected bacterial TTI investigations were concluded to be confirmed, probable
or possible. Three investigations were concluded to be near misses, with Staphylococcus aureus
identified in all cases.
Case 24.1: Near miss identified prior to issue to a patient (Staphylococcus aureus)
Staphylococcus aureus was cultured from a visually abnormal pooled platelet unit. The unit was tested and released as negative to date with no visual abnormality. Routine bacterial screening remained negative. The hospital noted a visual abnormality described as a white deposit in the two-day-old platelet pack prior to transfusion. The unit was returned and cultured, with Staphylococcus aureus identified. Associated units were discarded; there was no patient harm. All four donors were followed up and nasal swabs taken. One donor was carrying Staphylococcus aureus; however, this was a different strain to that cultured from the pack. This donor has been withdrawn from donation.
Case 24.2: Near miss identified through presence of aggregates in apheresis platelets (Staphylococcus aureus)
Bacterial growth of Staphylococcus aureus was confirmed following identification of aggregates in apheresis platelets (2 splits) prior to issue. Initial BacT/ALERT platelet screening was negative. There was no patient impact, as no components were transfused.
Case 24.3: Near miss identified through presence of aggregates in pooled platelets (Staphylococcus aureus)
Growth of Staphylococcus aureus was confirmed following identification of aggregates in a platelet pool, prior to issue. Initial BacT/ALERT platelet screening was negative; the platelet pool was positive when retested. Three associated red cell units and one plasma-for-medicine component were available for recall and testing; all were negative. One red cell unit had been transfused, but following clinical review no transfusion reaction or illness in the patient was noted.
Learning point
- The near‑miss bacterial transfusion‑transmitted infections highlight the ongoing importance of visual checks of blood components, especially platelets, before issue and administration, as inherent risk remains despite continuous BacT/ALERT cultures throughout the platelet lifespan.
Baterial TTI 1996-2025
Since reporting began in 1996, a total of 40 confirmed incidents of bacterial transfusion-transmissions to individual recipients have been reported. Of these, 33 have been caused by the transfusion of platelets, and 7 by red cells. One red cell case in 1998 also involved fresh frozen plasma (FFP) (Table 24.4). The most recent bacterial transmission was 2015. The introduction of bacterial screening has had a significant impact on the numbers of bacterial TTI; however, platelet packs are issued as ‘negative-to-date’ and reactivity post issue will result in recall. It is known that results may be falsely negative, particularly in cases involving Staphylococcus aureus.
Between 2011 and 2025, 13 near misses have been reported in platelet components, with one additional case in red blood cells. In 12 of the 14 cases, the species identified was Staphylococcus aureus. Current British Society for Haematology (BSH) guidance recommends that patients are advised to report any symptoms that occur within 24 hours of transfusion although patients with confirmed bacterial TTI generally become unwell very rapidly, often during transfusion (Soutar, et al., 2023). Clinical teams are reminded that any suspected bacterial TTI should be discussed with the relevant Blood Service so that, if appropriate, packs can be returned for culture and any other associated packs recalled.
Viral and parasitic TTI reports in 2025
In 2025, there were 10 suspected viral and parasitic TTI investigated. Six investigations were concluded as no transmission, 1 possible HBV and 1 undetermined HBV were concluded; investigations are pending for 1 malaria and 1 HBV suspected transmission. UK Blood Services may be asked to ascertain the cytomegalovirus (CMV) risk in retrospect from blood components that have been used in an emergency and where normally CMV IgG negative units would be requested. These investigations are not covered in this chapter as they do not meet the definition of a TTI, they are described in Chapter 10, Incorrect Blood Component Transfused (IBCT).
Update on viral TTI investigation reports from 2024
Of the 3 pending investigations reported in 2024, the HCV was concluded as no transmission, the parvovirus B19 (B19) was concluded as a probable transmission, and there is an additional B19 investigation that is still pending, awaiting archive testing results. The probable B19 investigation involved a kidney transplant recipient with multiple donor exposures, including seven red cell units, four units of FFP, two units cryoprecipitate and one pooled platelet component. The recipient received red cells for anaemia following the transplant and was subsequently diagnosed with high grade parvovirus two months later. Archive testing of the donors identified one was positive for B19. This was prior to testing of all whole blood and plasma donors for B19 in England and Scotland. Molecular typing was not carried out, but the transfusion was the most likely source of the transmission.
Confirmed viral TTI 1996-2025
The year of transfusion may be many years before an incident is investigated and/or reported to SHOT due to the chronic nature, and possible late recognition, of some viral infections. Since 1996, 33 confirmed transfusion-transmitted viral infections have been documented in the UK, most commonly HBV (n=11) and HEV (n=12). HBV cases are more frequently reported because acute infections in donors may not be detected due to the longer HBV assay window period, and occult HBV can escape detection when very low deoxyribonucleid acid (DNA) levels fall below the limit of nucleic acid testing (NAT). The introduction of pooled NAT in 2009 and anti-HBc screening in 2022 has reduced this risk. HEV, despite having a shorter window period, is more frequently detected in donors because it is generally acquired through food and there is no specific donor selection to exclude those at risk, leading to higher HEV ribonucleic acid (RNA) prevalence and a greater chance of non‑detection and transmission.
Other reports
Not all reports proceed to a full investigation if transmission can be ruled out, as in some examples below.
- If a recipient tests positive for only antibodies to infection, it is possible that passive transfer of antibodies has occurred due to receipt of intravenous immunoglobulin. If this is suspected, repeat testing should be carried out four to six weeks after the transfusion date. If this is due to passive transfer of antibodies, then reactivity should have resolved within this time.
- In recipients where only IgM antibodies are detected, reactivity for RNA/DNA and seroconversion (e.g., IgG) would also need to be confirmed before TTI investigations commenced. IgM assays are often cross-reactive and non-specific, so isolated IgM reactivity is not usually diagnostic.
- In recipients with evidence of a chronic infection, previous negative results may help rule out reactivation under immunsupression and assess whether transfusion is the most likely source of infection.
- For older cases of possible TTI, year of transfusion should be provided for the implicated transfusions in addition to the unit numbers to enable effective investigation by the Blood Services.
Residual risk of HBV, HCV, or HIV
The chance, or residual risk, of a potentially infectious HBV, HCV or HIV window period donation not being detected on testing in the UK are estimated to be very low at less than one per million donations tested (Table 24.2) (JPAC), 2024a). These estimates reflect the level of infection in blood donors and the duration of the window period for the assays in use. The window period is the time very early in the course of infection when tests in use do not detect the virus but there may be a sufficient amount for transmission and is highest for HBV at 30 days. The calculations are made annually, but for HBV only consider the risk of non-detection of acute infections and not the risk of non-detection of an occult hepatitis B infection (OBI). The residual risk of HEV is not routinely calculated but has been previously estimated to be considerably higher than for HBV, HCV, or HIV (Harvala, et al., 2022).
Table 24.2: The estimated residual risk that a whole blood donation made in the infectious
window period is not detected on testing: Risks specific for HBV, HCV and HIV, UK 2022 to 2024
| HBV | HCV | HIV | |
|---|---|---|---|
| Number per million donations | 1.09 | <0.01 | 0.1 |
| 95% confidence interval | (0.63-3.35) | (0.00-0.09) | (0.04-0.28) |
| At 1.8 million donations per year, testing will miss a potentially infectious window period donation every: | 0.5 year | 50 years | 6 years |
Far fewer TTI are observed in practice than the estimated risks in Table 24.2. This may be partly due to the fact that the estimates have wide uncertainty, and the model used to calculate risk is based on the risk in all whole blood donations tested. The model does not incorporate non-use of packs, recipient susceptibility to infection, or under-ascertainment/under-reporting. Examples include recipients dying from an underlying medical condition before a chronic asymptomatic viral condition is identified, or, in the case of HBV, an asymptomatic acute infection.
Blood donation testing and surveillance
Every blood donation in the UK is tested for markers of HBV, HCV, HEV, HIV, HTLV (for new donors and non-leucodepleted products for England and Scotland, and testing of all donors for Northern Ireland and Wales) and syphilis, with some donations also tested for malaria, Trypanosoma cruzi and West Nile Virus (WNV), depending on donor history. Information about donations tested and donors found positive is carefully monitored to help assure safety for recipients (NHSBT and UKHSA, 2025). Anti-HBc screening for blood donations was rolled out as part of routine screening across the UK in 2022 in response to a review carried out by the advisory committee on the Safety of Blood, Tissues and Organs (SaBTO), to reduce the risk of HBV transmission from donors with occult HBV (Department of Health and Social Care, 2023) (SaBTO, 2023). This increased the detection of potentially transmissible HBV from donors with OBI, which have been removed from the blood supply.
HEV NAT screening of apheresis donations was changed from pooled to individual donations for Wales from November 2022, for Scotland from April 2024 and Northern Ireland from November 2024. A recent SaBTO review on the current HEV screening of blood and apheresis platelet donors recommended that continuing with the with current screening in minipools is appropriate (Department of Health & Social Care, 2025). Real-time screening of donations of plasma for medicine has been carried out for markers of HAV and parvovirus B19 since April 2025 in England and for all donations in Scotland.
Lookback investigations
Lookback investigations are initiated by the UK Blood Services when repeat donors are found to be newly positive for a marker of infection, either due to donor seroconversion, post-donation information or introduction of new test. These investigations will usually involve contacting hospital teams to ascertain the fate of the units and and follow up of the recipient.
In 2025 two lookback investigations were initiated in England in repeat donors with newly identified markers. One apheresis donor, whose most recent donation was HEV RNA positive, was picked up on pooled sampling. The archived sample from the most recent screen negative donation was positive, picked up by individual NAT. Two recipients were traced; one was deceased and one was tested with no evidence of infection. The other donor had markers of occult hepatitis B, this donor had donated three times previously, no archived samples were available for testing. Five recipients who had received these donations were followed up; four recipients were deceased, one tested with no evidence of infection. In Scotland, ten syphilis and one HEV lookback investigations were conducted, with no transmission identified.
Emerging infections
Horizon scanning is performed by UK Blood Services to identify new and emerging pathogens which may threaten the safety of donated products, and to ensure that appropriate actions are taken to mitigate any risk identified. The Emerging Infection Report (EIR) produced by the NHSBT/UKHSA Epidemiology Unit is distributed to Joint United Kingdom (UK) Blood Transfusion and Tissue Transplantation Services Professional Advisory Committee (JPAC) Standing Advisory Committee on Transfusion-Transmitted Infections (SACTTI) on a monthly basis with items escalated sooner as needed. The EIR is reviewed by SACTTI and may lead to further risk assessment and changes to the donor selection guidelines, or other blood safety measures, where necessary (JPAC, 2026).
Variant Creutzfeldt-Jakob disease (vCJD) 2025
There were no vCJD investigations in 2025.
vCJD 1996-2025
Three historic vCJD incidents took place prior to the introduction of leucodepletion in 1999 and prompted a range of other measures taken by the UK Blood Services to reduce the risk of vCJD transmission by blood, plasma, and tissue products. All these measures have been reviewed and endorsed by SaBTO (Department of Health and Social Care, 2013).
The most recent vCJD case was in 2016 and not found to be a donor. Specific funding for CJD surveillance in transfusion medicine, formally named the Transfusion Medicine Epidemiology Review (TMER) ended on 31 March 2025. The surveillance ran for 28 years and found no evidence up to that time of sporadic CJD transmission via the blood supply (JPAC, 2024b). UKHSA are now responsible for UK CJD surveillance. CJD has been made a notifiable disease in England, and all suspected or confirmed cases must be reported immediately to UKHSA through Notifications of Infectious Diseases (NOIDS).
Diagnostic testing continues to be provided by the University of Edinburgh via referrals to the National Prion Clinic in London. Any new vCJD case identified in a donor would trigger a lookback investigation. Several countries – including Australia, Canada, Republic of Ireland, Switzerland and the US – have removed blood donor deferrals for individuals who have lived in the UK between 1980 and 1996, and the Food and Drug Administration (FDA) has also lifted the deferral for those who have received a transfusion in the UK since 1980 (FDA, 2022; Hoad, et al., 2023; AABB, 2026).
Table 24.3: Number of confirmed TTI incidents, by infection in the UK, reported to SHOT, with transfusions between October 1996 and December 2025 (Scotland included from October 1998)
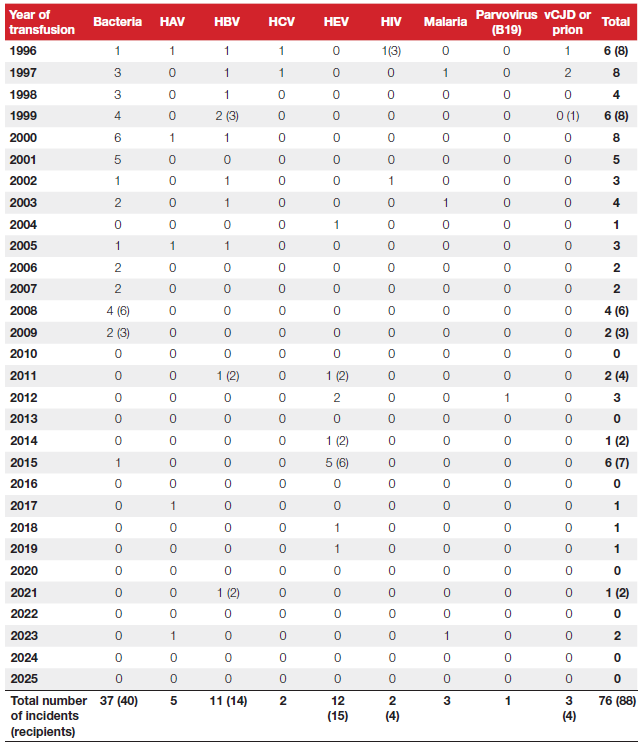
Table 24.4: Number and type of implicated components from confirmed TTI recipients in the UK, reported to SHOT, with transfusions between October 1996 and December 2025 (Scotland included from October 1998)
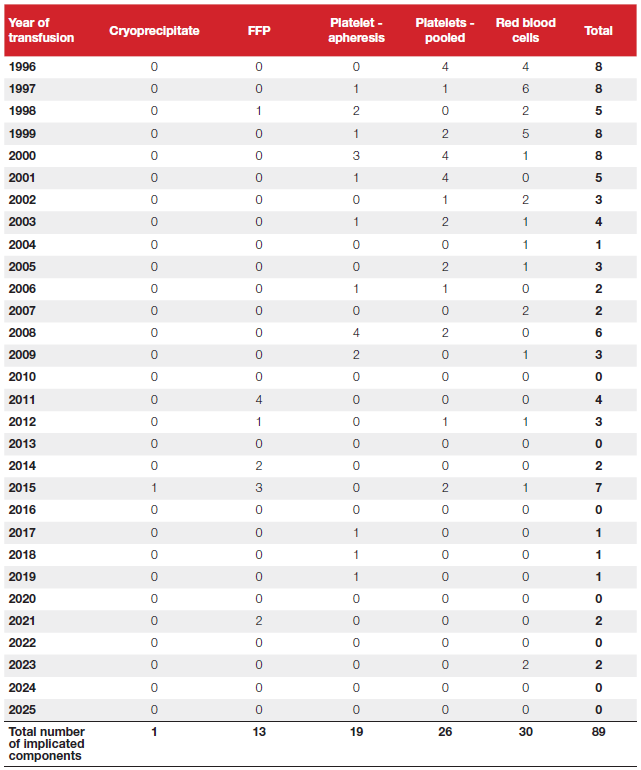
Table 24.5: Outcome of confirmed TTI incidents (and recipients) and implicated components by infection in the UK, reported to SHOT, with transfusions between October 1996 and December 2025 (Scotland included from October 1998)
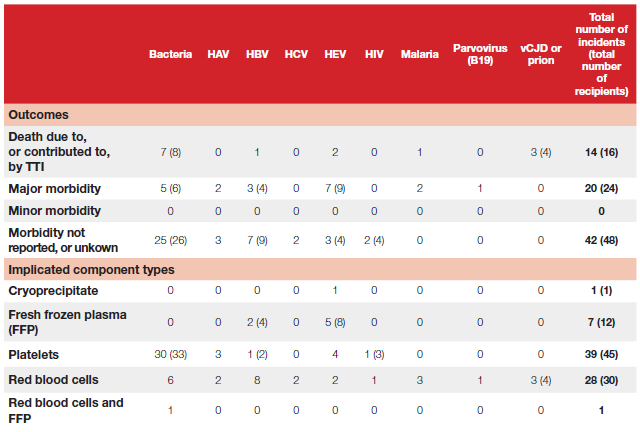
Accompanying notes for Tables 24.3, 24.4 and 24.5:
- TTI of HCV, HEV, HIV or HTLV identified either before routine screening or through national lookbacks following the implementation of screening are recorded separately and do not form part of the main Annual SHOT Report numbers.
- Where applicable, number of recipients are included in brackets.
- The year of transfusion may be prior to year of report to SHOT due to delay in recognition of chronic infection.
- To the end of 2025, no routine blood donation screening has ever been in place for vCJD, although other safety measures are in place (Department of Health and Social Care, 2013).
- In 2004 there was an incident involving contamination of a pooled platelet pack with Staphylococcus epidermidis, which did not meet the TTI definition because transmission to the recipient was not confirmed, but it would seem likely. This case was classified as ‘not transfusion-transmitted’.
- During 2025 HAV and parvovirus (B19) screening was implemented by England and Scotland to facilitate collection of plasma for fractionation.
- HCV investigations where the transfusion was prior to screening are not included in the above table.
- HEV RNA screening in the UK began with selective testing from 2016, followed by universal screening from April 2017, and was not in place at the time of the documented transmissions.
- The two early HIV incidents (pre-1996 and in 1996) were associated with window period donations (anti-HIV negative/HIV RNA positive) before HIV NAT screening was in place. A third window period donation in 2002 was transfused to an elderly patient, who died soon after surgery. The recipient’s HIV status was therefore not determined and not included.
- HTLV screening began in 2002.
- In the early malaria transmissions (1997, 2003), malaria antibody testing was not applicable at the time according to information supplied at donation.
- The vCJD case in 1999 was found to have the same blood donor as one of the 1997 transmissions and has therefore been counted as the same incident. Please note this was counted as two separate incidents in previous reports.
- A further prion case died but transfusion was not implicated as the cause of death. The outcome was assigned to major morbidity instead because although there was post-mortem evidence of abnormal prion proteins in the spleen, the patient had died of a condition unrelated to vCJD and had shown no symptoms of vCJD prior to death.
For further information or alternative breakdown of data please contact the National Coordinator for Transfusion Transmitted Infections via the NHSBT/UKHSA Epidemiology Unit at [email protected]
Learning points
- Visual inspection of blood component packs throughout the transfusion pathway helps reduce TTI.
- The UK Blood Services also investigate suspected TTI for agents that are not routinely screened for.
- Lookback investigations are rare, and the UK Blood Services appreciate collaboration to support the work involved in identifying the fate of donated blood components.

Conclusion
Investigations of 110 reports of possible TTI in 2025 resulted in no confirmed transmissions (bacterial, viral or parasite). This provides assurance of the safety of the UK blood supply as a result of the effective measures and haemovigilance systems in place to reduce TTI. Policies and procedures are constantly reviewed to see if any other mitigations are required.
Despite mitigation strategies to reduce the risk of bacterial contamination, Staphylococcus aureus near miss events remain a challenge to the safety of the platelet supply. These events account for 74% of near miss events identified since surveillance started in 1996, and 86% since the rollout of platelet screening in 2011. Staphylococcus aureus is recognised as a bacterium of clinical significance, associated with the last TTI identified in the UK in 2015. This is further compounded by its slow-growing nature which can escape detection (Matsumoto, et al., 2022).
The near‑miss cases investigated in 2025 highlight the need for sustained vigilance and provide important evidence for maintaining robust haemovigilance of the blood supply.
Recommended resources
Number of recipients with confirmed/probable Transfusion-Transmitted Infections (TTI)
SHOT Bite No.07a: Reporting and investigating bacterial Transfusion-Transmitted Infections
(TTI)
SHOT Bite No.07b: Reporting and investigating non-bacterial Transfusion-Transmitted
Infection (TTI)