Authors: Rebecca Elder and Claire Wroe
Link to PDF chapter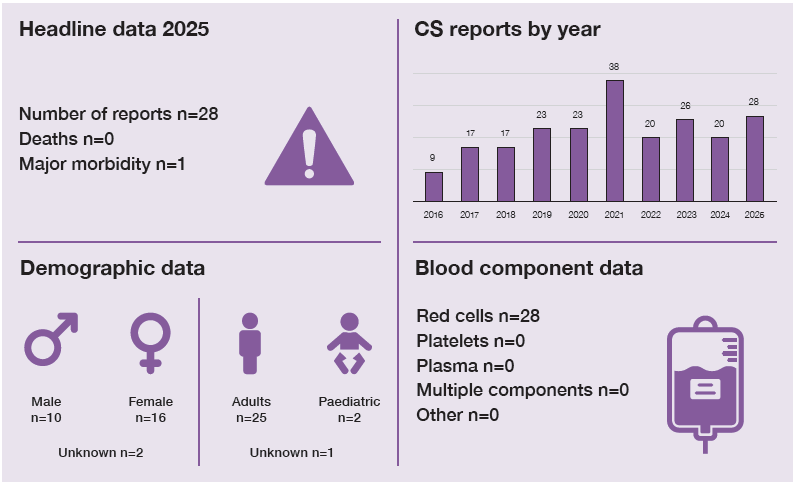
Key SHOT messages
Key findings
- The small number of cell salvage reports prevents meaningful generalisation and limits the identification of recurring safety themes.
- Avoidable procedural errors remain the most prevalent incidents reported.
Gaps identified
- Inconsistent use of intravenous (IV) saline has been identified, highlighting the need to avoid the use of irrigation saline.
- A better understanding of the contribution of human factors to preventable errors in cell salvage is needed to inform improvement actions.
Good practice
- Several procedural errors were supported locally by the roll-out of education and support for training issues.
- Appropriate corrective and preventive actions were reported following local incident investigations in a few cases.
Next step
- Organisations are encouraged to include cell salvage within local transfusion safety reporting processes and to report all associated incidents to SHOT in accordance with national and local guidance.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Cell salvage definition
Any adverse events or reactions associated with cell salvage (autologous) transfusion methods, including intraoperative and postoperative cell salvage (washed or unwashed).
For a more detailed definition see https://www.shotuk.org/reporting/incident/definitions/
Introduction
In 2025, 28 cases were included, which is consistent with previous years: but there is evidence of potential under-reporting (Kumar, et al., 2024).
The SHOT Transfusion Safety Standards set clear expectations for safe transfusion practice through strong haemovigilance, governance and learning from incidents and near misses. They support Patient Blood Management by promoting measures such as cell salvage to reduce avoidable transfusion and associated harm. Using learning from safety incidents to inform improvement actions is essential to strengthen systems and enhance transfusion safety across the pathway (SHOT, 2025b).
Reports were submitted by 20 different organisations; one centre submitted 6 reports, one submitted 3 reports, and another submitted 2 reports; the remaining 17 reporting sites submitted a single report each. One incident was withdrawn from the final total as it did not meet the reporting criteria. Two cases involved paediatric patients; one was an adverse reaction, and the other was an equipment error.
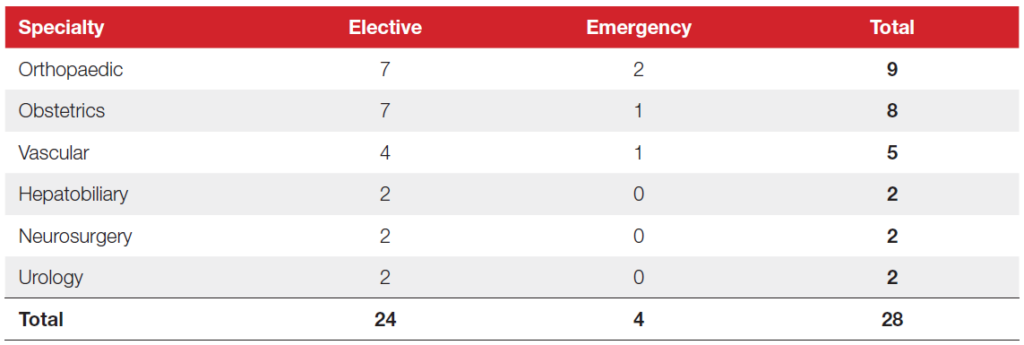
Most reports involved patients undergoing elective surgery, 24/28 (85.7%). More than half the events were reported from orthopaedic and obstetric surgery, with remaining reports occurring in six different specialities. All incidents were related to the intraoperative use of centrifugal washing devices.
Table 25.1: Cell salvage cases by specialty in 2025 (n=28)
| Specialty | Elective | Emergency | Total |
|---|---|---|---|
| Orthopaedic | 7 | 2 | 9 |
| Obstetrics | 7 | 1 | 8 |
| Vascular | 4 | 1 | 5 |
| Hepatobiliary | 2 | 0 | 2 |
| Neurosurgery | 2 | 0 | 2 |
| Urology | 2 | 0 | 2 |
| Total | 24 | 4 | 28 |
OR
There were 24 adverse events, 13 of which were attributable to avoidable errors, and 11 machine/disposable failures. There were 4 adverse reactions. Avoidable errors were the most reported incident.
Deaths related to transfusion n=0
There were no deaths related to cell salvage.
Major morbidity n=1
The patient, who was undergoing vascular surgery, became hypotensive following infusion of cell salvaged blood (no leucocyte depletion filter (LDF) was used), requiring postoperative vasopressor support. The investigation deemed that reinfusion of cell salvaged blood was responsible for the hypotension; however, the patient also returned to theatre for investigation of a suspected arterial bleed. The patient required adrenaline and vasopressors, had a short critical care admission, and recovered as expected.
Cell salvage adverse events n=24
There were 11 incidents related to machine/disposable failure, with an additional 13 avoidable procedural errors.
Equipment failure n=11
There were 11 reports of equipment failure, 4 of which were reported to the Medicines and Healthcare products Regulatory Agency (MHRA) under the Yellow Card scheme. Four incidents were attributed to the age of the machine, despite devices being on maintenance contracts.
There were 3 device malfunctions, with 2 sensor faults and 1 software failure. Six incidents related to cell salvage consumables. One device was rendered unusable as a drip pole became detached. In most cases, measures were taken to minimise consequences to the patient by continuing cell salvage or sourcing an alternative machine. One patient received an allogeneic blood transfusion, which potentially would not have occurred otherwise, and one machine was rendered unusable, but the patient did not require an additional transfusion.
One hospital raised an incident following the formation of a frothy deposit around the collection reservoir. Salvaged blood was transfused uneventfully despite this. Limited information was available from the local incident investigation and SHOT have not received any similar reports regarding manufacturing faults affecting consumables.
Learning points
- Reporting incidents safeguards patients through vigilant monitoring of equipment.
- Maintenance contracts must meet service expectations, to avoid operational challenges and patient safety issues.
Procedural errors n=13
There were 3 reports where saline (0.9% sodium chloride) for irrigation was used instead of IV saline. Saline for irrigation may differ from IV saline in terms of sterility, purity and pH and is not intended nor licensed for IV use. In 1 case, the incorrect preparation was recognised and discarded, with no effect on the patient; in another, the incorrect preparation was used to wash swabs and transfused back into the patient, no clinical reaction, remained stable post operatively; and in another, saline for irrigation was used with cell salvage suction and the collected blood had to be discarded.
Saline for irrigation is widely available in bags or bottles and can be connected to irrigation or poured directly from the container. They are labelled as ‘For irrigation only. Not for injection’.
Without robust system supports, reliance on human vigilance, even with two‑person checks, remains vulnerable to error. In response to the incident involving transfusion of irrigation saline, one hospital removed all irrigation saline from theatres, updated local policy, and appointed an interim cell salvage lead.
Similar errors were also reported with other IV fluids. In 1 case, IV compound sodium lactate (Hartmann’s) was used instead of saline during cell salvage. In another, a sterile IV‑grade saline bag was inadvertently desterilised using non‑sterile scissors and poured onto a swab, but this was recognised and discarded before any harm occurred.
Data from previous Annual SHOT Reports highlights the incorrect use of saline in intraoperative cell salvage is a recurring error. Guidance is clear that red blood cells collected during cell salvage must be washed using intravenous normal saline at a concentration of 0.9% sodium chloride, with the final product being the patient’s own red blood cells suspended in this solution for reinfusion (UKCSAG, n.d.).
Learning points
- Ensure saline for irrigation is clearly segregated from IV fluids, as similarities in appearance can lead to incorrect use.
- Clear labelling (‘For irrigation only. Not for injection’) alone does not remove risk; environmental layout, storage practices and workflow are additional factors influencing selection errors.
Case 25.1: Loss of salvaged blood as a result of untrained operator and procedural issues
A patient (known to be anaemic) underwent elective obstetric surgery, with planned cell salvage. The surgery was described as ‘difficult’, with 2 litres of intraoperative blood loss. Half a litre of blood was salvaged; however, an incorrect procedure followed during machine disconnection resulted in the blood bag having to be discarded.
The salvaged blood was wasted, and the cell salvage machine removed from service and deep‑cleaned due to contamination from mishandling. The staff member involved was not trained in cell salvage; training and clinical supervision were arranged afterwards. While this prompt response was positive, the patient’s anaemia, the challenging surgery, and significant haemorrhage raise concerns about why an untrained staff member was operating cell salvage without support. It is not fully known whether the situation could have been anticipated, or whether the departmental support structures were adequate. Several other incidents also revealed retrospective identification of training gaps, highlighting the importance of competency assessment.
In another case, an operating department practitioner (ODP) operating cell salvage went for lunch, and the relief ODP lacked familiarity with cell salvage for aneurysm repair, delaying surgery. Training was addressed through a refresher course and development of a vascular surgery cell salvage guideline. This reinforces the importance of recognising skillsets, working within capability, and ensuring safe handover, particularly when staff work dual roles such as ODP and cell salvage operator.
Case 25.2: Metallosis in revision hip surgery and impact on cell salvage
A patient underwent an elective revision of hip replacement due to trunnionosis (a complication of hip arthroplasty from the mechanical wear and corrosion of the femoral head-neck interface, causing the release of metal debris). Preoperative imaging revealed debris, but metal specific blood tests were not carried out. The orthopaedic team anticipated that the issue was ceramic joint failure. Cell salvage was scheduled; however, metal debris was noticed on collection and collected blood was discarded appropriately. This correlated with markedly raised metal-specific blood tests postoperatively.
This case represents a near miss due to theatre staff vigilance. Whether this could have been anticipated preoperatively is unclear, however the use of cell salvage is becoming more common in revision hip surgery, and it is important to exercise caution where there is a risk of metal debris.
There is no clear evidence regarding whether cell salvage is effective in removing metal debris. Reijngoud, et al. (2009) reported that >70 percent of metal debris is removed using cell salvage, although advised caution with its use. Some companies manufacture a specific collection reservoir with a filter designed to catch metal debris or recommend the use of a LDF in reducing transfused debris. It may be that these methods are reserved for cases where cell salvage is unavoidable or following a risk benefit assessment.
Case 25.3: Environmental factors result in unplanned allogeneic transfusion
A patient underwent elective surgery, with cell salvage performed by an ODP working in a dual-operator role using both cell salvage suction and a surgical waste management suction system. The ODP’s view of the suction and cell salvage reservoirs was obstructed by the patient, surgeons, scrub staff and equipment. The team lost track of blood loss until the patient became symptomatic. The ‘wrong’ suction was used for blood loss, and so there was an inadequate volume of blood in the cell salvage reservoir, and the patient required allogeneic blood transfusion.
This case reflects more than an individual error and demonstrates how human factors such as environmental layout, situational awareness, and team vigilance contribute to incidents. Recognising the multifactorial pressures faced by cell salvage providers, particularly when working as dual operators, would assist in providing appropriate support for the service and to promote learning within a just, non‑punitive culture.
One incident detailed how >300mL of salvaged blood was discarded due to a prolonged transfusion time secondary to a painful cannula and was met with an education session focussing on reinfusion of blood. Another incident described how 1.5 litres of salvaged blood was reinfused without adherence to local safety checks. This was addressed with education and signposting towards the hospitals policy documentation.
One organisation reported excessive clotting within the collection bowl when moving to a single suction technique for amniotic fluid and blood. Reverting to the previous technique of using two separate suctions has resolved the issue. This issue has been raised verbally by some independent operators (but not reported to SHOT), and may represent issues with anticoagulation dosing, requiring additional training. This demonstrates the importance of incident reporting to SHOT to allow the identification of trends and for early intervention and support with recurring issues.
One case was cancelled due to staff not being able to operate the cell salvage machine.
Learning points
- Effective learning from cell salvage safety incidents requires the application of human factors principles to shape targeted improvement actions.
- All staff involved in cell salvage must be appropriately trained and assessed as competent in relevant tasks to ensure safe processes and protect patient safety.
- The UK Cell Salvage Action Group (UKCSAG) has devised a standardised training framework and competency assessment (UKCSAG, n.d.).
Cell salvage adverse reactions n= 4
There were 4 reports of adverse reactions. One comprised of haematuria following transfusion of allogeneic and autologous blood, attributed to mechanical haemolysis (not a transfusion reaction).
Three cases reported hypotension on reinfusion of salvaged blood. In 1 case, it was initially thought to be due to acid citrate dextrose anticoagulant, but the postoperative investigation attributed hypotension to the clinical condition of the patient. Another case is described in the major morbidity section. In the final case, reinfusion of cell salvaged blood coincided with an epidural top-up and the patient became hypotensive, requiring vasopressor support. After stabilisation, the hypotension recurred on restarting the reinfusion of blood.
Learning point
- Hypotension following reinfusion of cell salvaged blood frequently has multiple contributing factors. These should be managed by reviewing the clinical situation while pausing reinfusion of salvaged blood to support accurate assessment and appropriate management.
Conclusion
Under-reporting of incidents affects the ability to risk stratify cell salvage as an alternative treatment to allogeneic blood. This may be due to a lack of awareness about SHOT, incident reporting and governance structures within hospital teams. SHOT is collaborating with the UKCSAG to address under-reporting.
Variable training continues to contribute to errors which highlights the need to standardise training across cell salvage practitioners. Refresher training should also be available to staff as appropriate. To standardise training nationally, UKCSAG have devised education and competency assessments.
Most incidents associated with cell salvage are preventable, and so by developing our understanding of underlying human factors driving errors, we aim to reduce similar incidents recurring. To support ongoing safety analysis and improvement, SHOT have expanded data collection for cell salvage events in 2026 to examine how human factors contribute to preventable incidents.
Recommended resources
Cell Salvage (CS) Cumulative Data page
SHOT Bite No.21: Cell Salvage (CS) – insights from SHOT reports
UKCSAG Technical Factsheet 12: Metallosis and Intraoperative cell salvage