Authors: Jonathan Massie and Joseph Sharif
Link to PDF chapter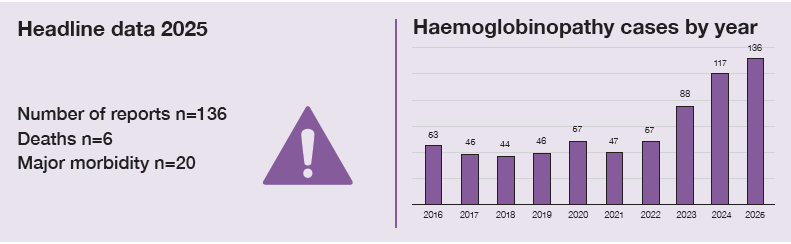
Key SHOT messages
Key findings
- Reports related to haemoglobin disorders continue to increase, mostly driven by reports of haemolytic transfusion reactions (HTR), incorrect blood component transfused-specific requirements not met (IBCT-SRNM) and delayed transfusions.
- There were 6 deaths related to transfusion: 1 related to delay, the other 5 related to HTR. There were no deaths with imputability 3 (definite).
Gaps identified
- Issues were more likely to be seen in cases where the patient was new to the hospital, being cared for by another team, or when transfusion was more urgent.
- Delayed or failed recognition of specific requirements is a frequent cause of delays and SHOT reports; all medical and laboratory staff need to be aware that haemoglobinopathy patients have specific requirements for transfusion.
Good practice
- There is increased reporting on the use of monoclonal antibodies as treatment for HTR, particularly in severe cases.
- Reports submitted to SHOT describe areas of good practice, such as prompt, appropriate treatment of transfusion reactions, highlighting that learning from incidents is taking place within local organisations.
Next steps
- During consent and shared decision-making for transfusion, patients with sickle cell disorder (SCD) should be informed specifically about the increased risk of alloimmunisation and HTR. This should include their potential implications for future transfusion.
- Clinicians should be familiar with the clinical features of HTR, including hyperhaemolysis, and ensure there are local protocols to support investigation and management.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Haemoglobin disorders definition
This chapter includes all incidents reported in patients with a significant haemoglobinopathy including sickle cell disorder and thalassaemia.
Introduction
The total number of haemoglobinopathy cases reported for 2025 was 136. Reports included 98 patients with SCD and 36 patients with thalassaemia. This represents an increase from 2024 (117 cases) and 2023 (88 cases).
SCD patients were most frequently represented in the HTR category. Thalassaemia patients were more commonly associated with IBCT-SRNM and delayed transfusions.
Table 27.1: Cases involving haemoglobin disorders reported in 2025 (n=136*)
| SHOT category | Sickle cell disorder | Thalassaemia | Total |
|---|---|---|---|
| HTR | 27 | 5 | 32 |
| IBCT-SRNM | 22 | 6 | 28 |
| Delayed transfusion | 15 | 6 | 21 |
| FAHR | 14 | 2 | 16 |
| TACO | 4 | 2 | 6 |
| Under or overtransfusion | 2 | 4 | 6 |
| NM | 3 | 3 | 6 |
| HSE | 2 | 3 | 5 |
| UCT | 3 | 2 | 5 |
| Avoidable transfusion | 3 | 1 | 4 |
| RBRP | 1 | 2 | 3 |
| Non-TACO pulmonary complications | 1 | 0 | 1 |
| Anti-D Ig errors | 1 | 0 | 1 |
| Total | 98 | 36 | 134 |
*There was 1 case of delayed transfusion in a patient with Diamond Blackfan anaemia, and 1 HSE case that involved multiple patients
Figure 27.1: Cumulative data for adverse transfusion events in patients with haemoglobin
disorders 2010 to 2025
Categories with 10 or fewer reports are included as ‘Other’
Deaths related to transfusion n=6
There were 6 deaths, of which 5 were related to HTR. Two of these cases were assigned imputability 2 (probable) and 3 were assigned imputability 1 (possible). A single death was reported as being related to delayed transfusion; this was assigned imputability 1 (Case 27.2).
Case 27.1: Delayed reaction after antenatal transfusion resulting in death (imputability 2 – probable)
A transfusion was arranged for a pregnant patient with SCD; they had no history of alloimmunisation or adverse transfusion reactions and had no other notable comorbidities. Post transfusion, they were initially well and returned home, but re-presented to hospital 10 days later with pain and dark urine. The patient was treated with further transfusion support, steroids, intravenous immunoglobulin (IVIg), eculizumab and plasma exchange, but developed multi-organ failure and died on the fourth day of admission. The working diagnosis was hyperhaemolysis or fat embolism syndrome.
Case 27.2: Delayed transfusion with pulmonary embolism (imputability 1 – possible)
A patient with SCD was admitted with generalised pain and acute kidney injury. The patient became particularly unwell on the evening of the third day of admission with parvovirus and an undiagnosed pulmonary embolism. Two units of red cells were prescribed, but there was a significant delay of around three hours in receiving the second unit despite the blood being available in the laboratory. The patient arrested shortly after transfusion of the second unit began. Subsequent review identified a delayed recognition of the need for blood as well as issues in communication and prioritisation. These issues contributed to the delay in transfusing this patient. Pulmonary embolism was identified as the likely cause of death at post-mortem, but it was possible that earlier transfusion would have improved the patient’s physiological reserve.
Major morbidity n=20
There were 20 cases associated with major morbidity in 2025. Of these 16 were in patients with SCD and 4 were in patients with thalassaemia. Reports involved HTR in 13 of the cases, 3 related to delays in transfusion, 2 related to TACO and 2 to FAHR (see Case 27.5).
Case 27.3: Multifactorial delayed transfusion in severe illness
A paediatric patient with SCD was transferred between hospitals to facilitate a red cell exchange transfusion for acute chest syndrome. They arrived in the evening and a sample for crossmatch was sent to the laboratory one hour later following a delay obtaining blood from the patient’s implanted port. Samples were sent via the pneumatic tube system, and the urgency of the sample was not communicated, meaning that the sample was not received by the transfusion laboratory for a further two hours. The sample was small, requiring a manual crossmatch which took further time. Additional delays occurred because there was a blanket requirement in the laboratory information management system (LIMS) for irradiated blood components for patients on the paediatric high dependency unit; however, this patient did not require irradiation. Clarification of this requirement and the subsequent manual issue of components resulted in the delay. Blood was therefore not available until eight hours after patient arrival during which the patient became more unwell and required intubation. The patient recovered after several days of intensive care unit (ICU) care.
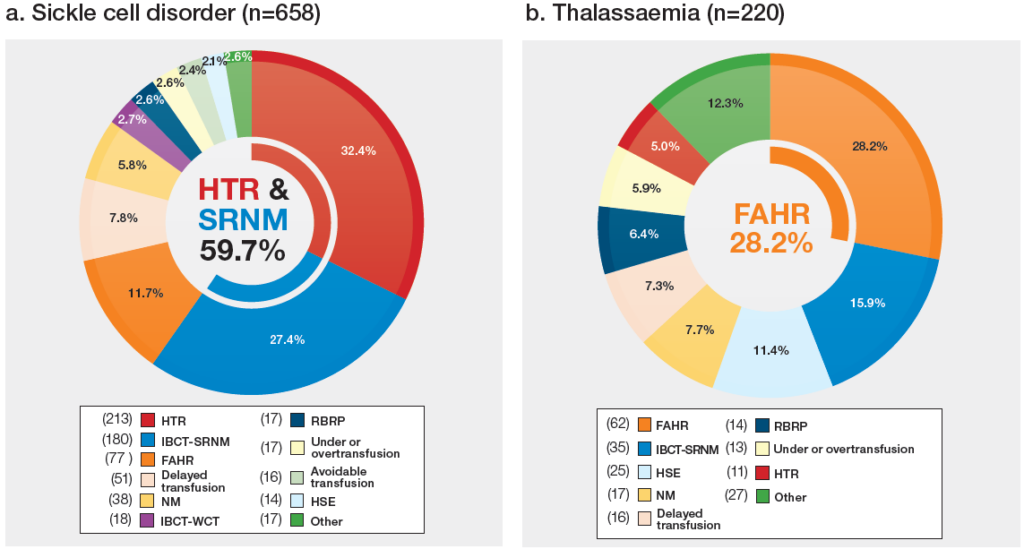
Haemolytic transfusion reactions n=32
There were 32 cases reported including 15 cases of hyperhaemolysis (HH), 15 delayed HTR and 2 acute HTR. SCD patients were involved in 27 of the cases and accounted for all 5 deaths related to HH. Of the 31 patients for whom prior antibody information was available, 10 had at least one specific alloantibody detected in the pre-transfusion sample, a further 6 had a history of previously detectable specific alloantibodies.
Treatment given included steroids for 23 patients, IVIg for 23 patients, erythropoietin (EPO) for 14 patients, eculizumab for 10 patients, tocilizumab for 2 patients and rituximab for 2 patients. One patient was treated with plasma exchange.
Case 27.4: Haemolysis following urgent blood transfusion without concessionary release
A patient with SCD was admitted to a hospital they had not previously attended for acute chest crisis. They required urgent transfusion; the antibody screen and direct antiglobulin test were negative, and red cells were crossmatched. An extended red cell phenotype had not been performed at their previous treating hospital and although an Rh phenotype had been performed in this organisation prior to transfusion, it was not used to guide decision-making due to anomalous results. Blood was released based on advice from haematology consultants without formal concessionary release. Following transfusion, the patient was found to have developed anti-C, and extended phenotyping was subsequently performed. Later in the year, the patient again received urgent blood without formal concessionary release. The patient developed severe haemolysis treated with IVIg, steroids, EPO and eculizumab. Additional alloantibodies (anti-S, -Kpa, -Fyb, and -Jkb) were detected in the post transfusion sample, posing increased lifelong transfusion complexity and risk.
Learning points
- Symptoms of haemolysis frequently begin outside of a healthcare setting; patients should be made aware of symptoms that might indicate haemolysis.
- Monoclonal antibodies, particularly eculizumab, are increasingly used in severe haemolysis, particularly hyperhaemolysis (NHSE, 2020b). In England, cases requiring eculizumab should be reported to the national haemoglobinopathy panel for retrospective approval.
- Differentiating between delayed HTR, hyperhaemolysis and other causes of haemolysis can be difficult. The British Society for Haematology guidelines on red cell transfusion in SCD give guidance on how to investigate (Davis, et al., 2017).
Febrile, allergic, and hypotensive reactions (FAHR) n=16
There were 16 reports of FAHR, 14 patients had SCD and 2 had thalassaemia. This contrasts with previous years where more patients who developed FAHR had thalassaemia. All but 1 of the cases was related to red blood cells, the other involved platelets. Of the 16 reactions, 10 were febrile and 6 were allergic in nature.
Case 27.5: Acute febrile reaction to red blood cells
A paediatric patient with SCD received 2 units of red blood cells. After the first unit, their temperature was 37.7°C and during the second it increased to 40.0°C. The transfusion was discontinued, and the patient was treated with paracetamol. A repeat group and screen sample was taken and it had a negative direct antiglobulin test result. The patient needed no further escalation of care and recovered completely from the febrile reaction.
This illustrates prompt and optimal management of a febrile reaction.
Learning point
- Treatment of febrile and allergic reactions should be targeted to the patient’s symptoms and signs (Soutar, et al., 2023).
IBCT-specific requirements not met n=28
There were 28 cases of specific requirements not met involving 67 units of red blood cells. These cases involved 6 thalassaemia patients and 22 SCD patients.
Patients with SCD or thalassaemia should receive red cells that are ABO-, Rh- and K-matched. Blood should be antigen-negative for any clinically significant red cell alloantibodies. Where the recipient is known to have SCD blood should be HbS-negative (Milkins, et al., 2013). Previously, it was recommended that blood should be <10 days old for top-up transfusion and <7 days old for use in exchange; please note that this recommendation has been removed (NHSBT, NBTC, UKTS and SCS, 2024). Age of blood recommendations for transfusion in these patients now only apply to children under one year of age.
Case 27.6: Error due to data sharing issues between partnered organisations
A patient with SCD attended for an elective top-up transfusion ahead of a planned surgery. The transfusion took place at the patient’s local hospital while much of their care was coordinated by a larger tertiary centre. The two centres were in a partnership, but specific requirements were not automatically shared and were instead communicated via an email inbox which was not checked daily. The local hospital’s laboratory was not aware that the patient had a diagnosis of SCD and therefore transfused blood that was not Rh- and K-matched.
Case 27.7: Wrong phenotype issued, missed opportunity to avert sensitising event
A patient with SCD with known alloantibodies (anti-S, -Jkb and -C) and a history of hyperhaemolysis presented in vaso-occlusive crisis and required an urgent top-up transfusion. The patient was found to have a pan-reactive antibody, meaning that samples were sent to the Blood Service reference laboratory. No new antibodies were found and a phenotype could not be carried out due to recent transfusion. The reference laboratory did not check previous genotype results, and four red cell units were issued which, although suitable for the patient’s known antibodies, were noted by the hospital laboratory to be incorrectly Rh-matched. The hospital laboratory identified the problem, and following discussions with the haematology consultant on call, the red cell units were given. The patient developed a new anti-E antibody.
Learning points
- Alloimmunisation and HTR are a significant risk of transfusion in haemoglobinopathy patients and in particular SCD. It is important to weigh up the risks and benefits of transfusion, the urgency, and the need to provide blood components that meet the requirements.
- Transfusion decisions in SCD and thalassaemia patients are inherently challenging and are further complicated during emergency situations. Careful assessment of the urgency of blood requirements is essential, and decisions should be reassessed if any concerns are raised.
Conclusion
There is often an assumption that patients with haemoglobinopathies will fully understand the nature and risks of transfusion. However, this cannot be known without taking the time to discuss these issues directly with patients. Several resources are available including patient information leaflets, which are regularly updated. These are supplemented by a range of new resources launched this year including the ‘My Transfusion’ app for patients, as well as a comic and picture book aimed at children (NHSBT, Hospitals and Science – Patient information leaflets, 2025b). As discussed in the recently updated consent guidelines, it is vital to involve patients in discussions around transfusion. This helps patients feel supported to question the process when something is wrong and feel confident in seeking support when complications arise (Murphy, et al., 2025). It is also essential that systems are robust enough to identify and safely manage these patients, particularly when care is provided in unfamiliar settings.
Data shows the disproportionate adverse impact of suboptimal shared-care pathways on patients with haemoglobinopathies. Safe shared care relies on multiple interconnected factors, including effective communication, well-informed staff, accurate documentation, and seamless interoperability of information systems. The UK National Haemoglobinopathy Register is making a positive impact on the quality of shared care information available.
It is hoped that broadening the blood donor base and introducing new technologies will support the provision of increasingly well-matched red cells. It is also encouraging that, when reactions do occur, clinicians now have access to more tools to manage them. Despite these advances, blood will continue to carry risks, not least because it is a biologically active, donated human substance rather than a manufactured commodity. Recipients are equally unique, and transfusion should always be an individualised intervention, with careful consideration of its necessity, regardless of whether the patient is regularly transfused.
Recommended resources
SHOT video: Meet the Experts – HTR & Haemoglobinopathies
SHOT Bite No. 24: Speaking up for safety
SHOT Bite No. 36: Shared care insights from transfusion incidents
