Authors: Vera Rosa and Susan Robinson
Link to PDF chapter Link to supplementary informationKey SHOT messages
Key findings
- Of the 73 cases received in 2025, 14 included women/birthing people with no previous pregnancies (NPP) and 59 with previous pregnancies (PP).
- D sensitisation still occurs when appropriate management of pregnancy is followed in accordance with national guidance.
- Live births in the index pregnancy accounted for 84% of cases, with 48% of babies requiring treatment for haemolytic disease of the fetus and newborn (HDFN).
Gaps identified
- Unnecessary administration of anti-D immunoglobulin (Ig) where immune anti-D was identified but not clearly communicated between the teams involved (clinical and laboratory) persists.
- Incomplete data sets continue to be submitted to SHOT, especially when previous pregnancies were managed outside the United Kingdom (UK) or in another healthcare organisation in the UK.
- Failure to refer maternal blood samples for quantification of anti-D can lead to inappropriate management of the pregnancy and impact the outcome.
- Data about management at birth for the index pregnancy is not currently collected, which is relevant when immune anti-D is identified beyond delivery (e.g., follow-up appointment).
Good practice
- In more than 50% of the cases reported in 2025, a cell-free fetal deoxyribonucleic acid (cffDNA) screening test was performed in the index pregnancy indicating an increased uptake of this test.
- A more proactive approach has helped increase the number of cases this year in which relevant information about key factors was provided, offering additional clinical insight.
Next steps
- Shared-care processes between healthcare organisations must be robust and accurate, with all relevant details regarding management of previous and/or current pregnancies regardless of the outcome.
- A national comparative audit took place between April and June 2026 to identify gaps in current practice and inform improvements. A report with findings is expected to be released in October 2026 and should be used to review local policies and processes.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Immune anti-D in pregnancy definition
Cases of D-negative pregnant women and birthing people who become sensitised and are found to have developed immune anti-D, which is detected during pregnancy, either at booking or later in the index pregnancy.
For a more detailed definition see SHOT Definitions
Introduction
The data collection of the cases reported under this category aims to understand the causes for D sensitisation. This category includes pregnancies managed in accordance with current guidance, in which biological factors may play a bigger role in the D sensitisation or where the pregnancy was not managed in accordance with current national guidelines. These include omitted or incorrect administration of anti-D Ig. The analysis of these cases can only be accurate, and the impact of each contributory factor correctly attributed, when the data set of the immune anti-D questionnaire is completed in full. Where information is not reported or not available, the interpretation of the contributory factors impacting that specific event might be incorrectly attributed and others more importantly missed. As in previous years, it was noted that these gaps are more likely to occur when the women or birthing people either access antenatal care (known as booking) late, have a prior pregnancy abroad or in the UK but in a different organisation. In this last instance, the unavailability of data highlights the current issues with shared care and information between National Health Service (NHS) and independent healthcare organisations emphasising the need for effective processes to improve patient safety.
Results
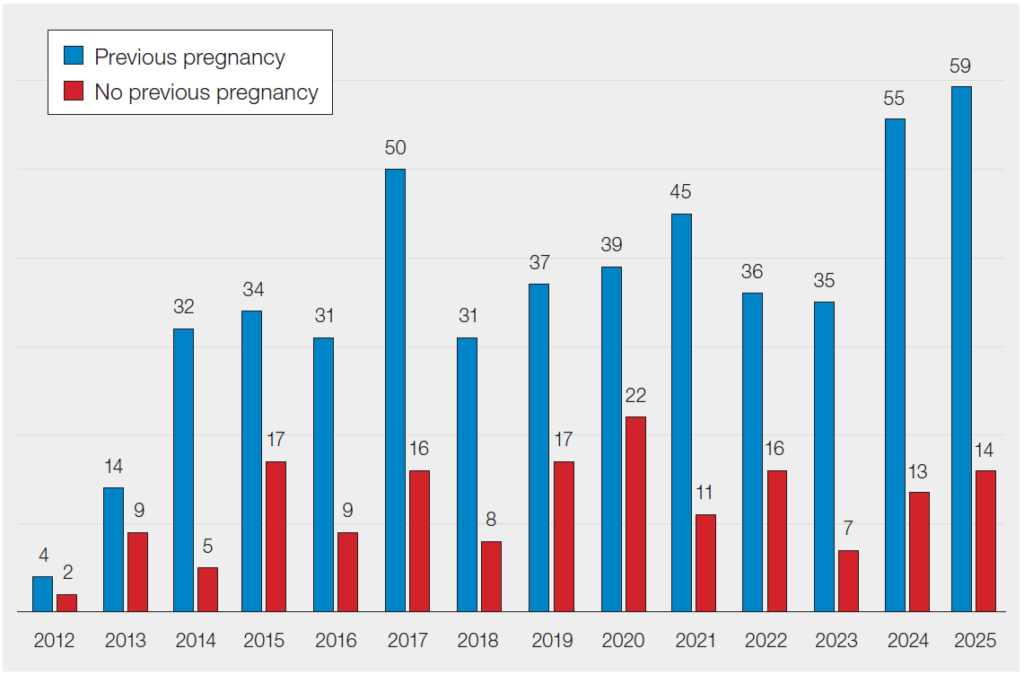
In 2025, SHOT analysed 73 cases of D sensitisation, in 14 immune anti-D was identified in the first pregnancy (NPP) and in 59 this antibody was detected in a further pregnancy (PP). A total of 166 NPP cases and 502 PP cases have been received since 2012 (Figure 29.1).
Figure 29.1: Number of SHOT reports of D sensitisation by year, 2012-2025
Contributory factors for D sensitisation such as body mass index (BMI), multiple pregnancies and management of index (current) and previous pregnancies, where applicable, continue to be analysed every year. In 2025, the BMI at booking was reported in 62/73 (84.9%) cases, of which in 23 the BMI was ≥30. Of these, in 8 cases the BMI was ≥40. A high BMI might result in a lower protective effect of the prophylaxis administered during pregnancy as the doses of anti-D Ig stipulated by the national guidelines are not weight specific (Qureshi, et al., 2014; Ngan, et al., 2024). Cases of multiple pregnancies (≥2) including miscarriages and termination of pregnancy (TOP) were identified in 34/59 (57.6%) PP cases ranging from 2 to 9 previous pregnancies. In cases of PP where immune anti-D was identified at booking, 22/59 (37.3%), the details of the immediate previous pregnancy might highlight the causes for D sensitisation assuming that no other relevant transfusion/transplantation history has changed between pregnancies.
A more proactive approach to the data analysis, including email reminders to provide pertinent details, has helped improve the number of cases this year in which relevant information about key factors, such as BMI, was provided, offering additional clinical insight.
Cases of no previous pregnancies (NPP) including no previous miscarriage or termination of pregnancy n=14
Figure 29.2: Summary of the 2025 NPP data (n=14)
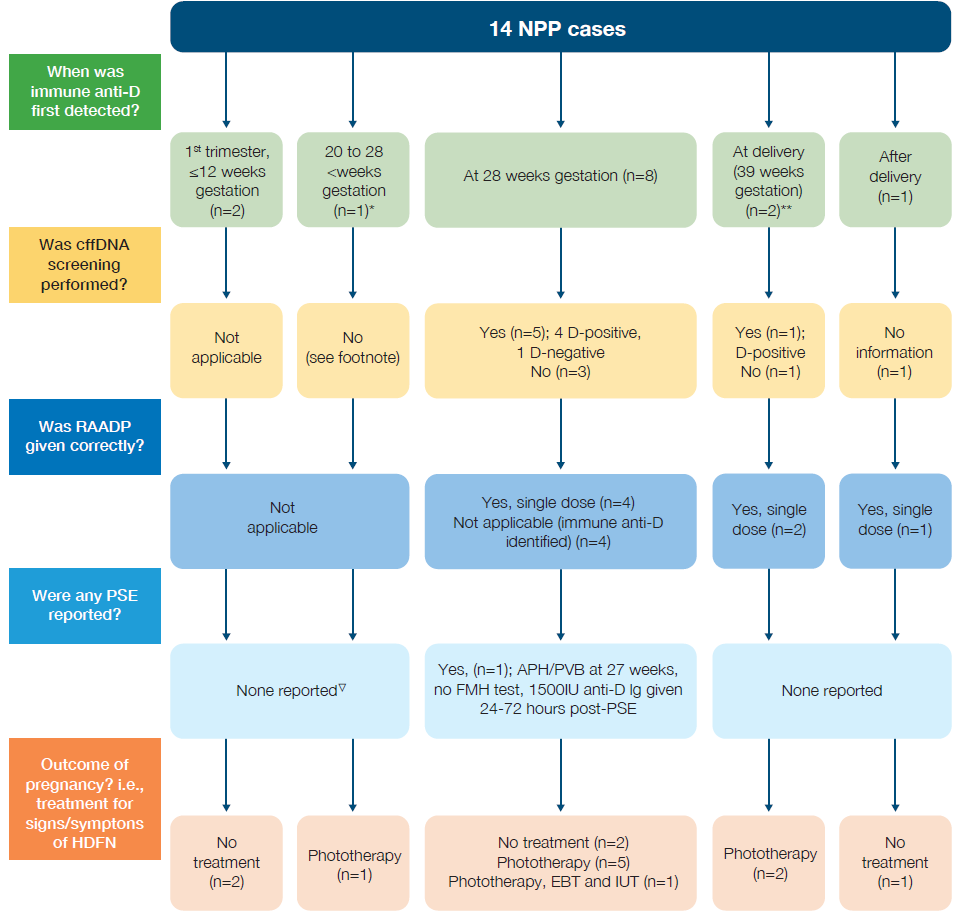
*Late booking – woman was first seen at 26+5 weeks gestation, when immune anti-D was identified
**Potentially identified at 28 weeks, however sample taken after anti-D Ig administration and not referred for quantification
▽First pregnancy, no PSE reported in early pregnancy and baby found to be D-negative at birth. No history of previous miscarriages or other PSE that could explain D sensitisation
Case 29.1: Unnecessary anti-D Ig administration with inadequate follow up
A woman with a normal BMI and in her first pregnancy was found to have immune anti‑D antibodies at 28 weeks’ gestation, with a quantification level of 0.7IU/mL. It was not documented whether she had received anti‑D Ig before the group and screen (G&S) sample was taken. At 30+5 weeks’ gestation, RAADP was offered and administered. No further samples were taken for repeat antibody quantification following this dose. The baby was born at 40+1 weeks’ gestation and required phototherapy postnatally.
Case 29.1 represents an example of unnecessary administration of anti-D Ig based upon:
- Communication – in most uncomplicated pregnancies it should be feasible to determine from records or discussion with the pregnant women or birthing people whether they had already received any anti-D Ig.
- The quantification level suggests the presence of immune anti-D i.e., >0.4IU/mL.
This case also represents a missed opportunity to follow up with repeat quantification at appropriate intervals to determine if fetal monitoring was required. According to the data provided, the D sensitisation occurred despite apparent appropriate antenatal care before antibody detection. The neonatal treatment required would not have differed in the presence of correct management.
Case 29.2: Unrecognised immune anti‑D and unnecessary anti‑D Ig administration
A woman in her first pregnancy and with a normal BMI received RAADP at 28 weeks’ gestation. A maternal G&S sample was taken 2 days after administration. Anti‑D was detected; however, the sample was not referred for antibody quantification. No further antibody monitoring was undertaken for the remainder of the pregnancy. Additional prophylactic anti‑D Ig was administered after birth. The postpartum G&S sample was sent for quantification, and the anti‑D level was reported as 77.3IU/mL. The baby was D‑positive, developed jaundice, and required phototherapy.
This case demonstrates a missed opportunity to obtain baseline samples prior to RAADP. There was also a missed opportunity to detect immune anti‑D, including appropriate quantification both before and after administration of RAADP. Earlier detection and monitoring could have influenced neonatal management and outcomes. The mother may have potentially avoided RAADP and certainly avoided anti-D Ig at time of birth.
Learning points
- Efforts taken to determine if anti-D Ig has already been administered in a pregnancy should include discussion with the pregnant person, checking medical health records, laboratory, and pharmacy records dependent upon local systems.
- Appropriate timing of maternal blood sampling prior to RAADP needs to be reinforced through education and should be included in decision-making pathways.
- When anti-D levels are quantified to be >0.4IU/mL, it is important to consider whether anti-D is likely to be immune especially in the absence of large doses of anti-D Ig (>1500IU). This needs to be included in staff education, reporting of results and is a relevant consideration when designing pathways prompts/clinical decision support.
Cases of previous pregnancies (PP) including miscarriages and terminations of pregnancy n=59
The index pregnancy in these cases refers to the current pregnancy; the pregnancy in which immune anti-D was first identified. The PP cases were separated into two different categories depending on the gestation when immune anti-D was first detected: ≤12 and >12 weeks gestation.
PP cases where immune anti-D was detected ≤12 weeks gestation (n=23)
Figure 29.3: Summary of the 2025 PP data where anti-D was detected ≤12 weeks (n=23)
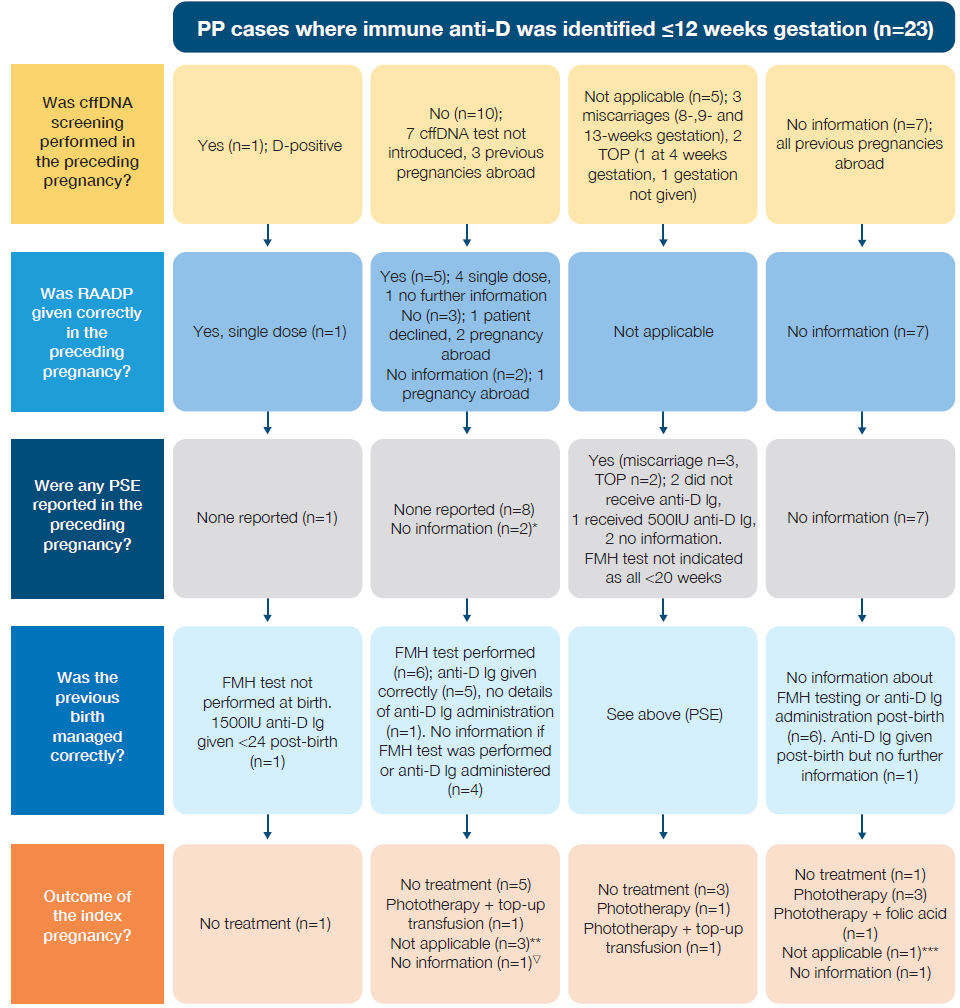
*1 case in previous pregnancy baby was found to be D-negative
**Outcome of index pregnancy: 1 miscarriage at 19 weeks, 1 TOP at 4 weeks, intrauterine death (IUD) at 26 weeks
***Outcome of index pregnancy: 1 miscarriage at 12 weeks
▽Patient moved abroad during pregnancy, unable to provide information about the outcome of index pregnancy
PP cases where immune anti-D was detected >12 weeks gestation (n=36)
Case 29.3: Severe HDFN following late detection of immune anti‑D
A woman with a high BMI and a history of two previous pregnancies outside the UK booked for antenatal care at 36+2 weeks’ gestation. An antibody screen identified immune anti‑D, with a quantification level of 71.04IU/mL. There was no record of anti‑D Ig administration in her previous pregnancies. The birth occurred at 37 weeks’ gestation. The baby was D‑positive and developed significant HDFN, requiring phototherapy, intravenous immunoglobulin (IVIg), and an exchange transfusion.
Women entering the UK who are considering pregnancy, or who are currently pregnant, should be encouraged to present early for appropriate antenatal management and early detection of potential risks. However, this can be challenging, and innovative approaches need to be considered to improve early engagement and access to appropriate care. These individuals are more likely to be sensitised if they had received a suboptimal standard of care including prophylaxis not offered in their country of origin. This may result in worse pregnancy outcomes, when presenting late, due to missed opportunities for increased surveillance and intervention/treatment decisions.
Learning points
- Information provided to women and birthing people coming into the UK who may be planning or indeed be pregnant should highlight that care may differ from their country of origin.
- Timely management and prompt presentation in early pregnancy ensure the best outcome for the mother/birthing person and the baby.
Details of 31/36 PP cases where immune anti-D was identified >12 weeks gestation are shown in Figure 29.4. In the remaining 5 cases the antibody was identified after birth i.e., immune anti-D was not present during pregnancy or at birth. In 3 of these, the antibody was identified at the postnatal follow-up appointment, 2 of which were following a large FMH volume at birth.

Figure 29.4: Summary of the 2025 PP data where anti-D was detected >12 weeks (n=31)
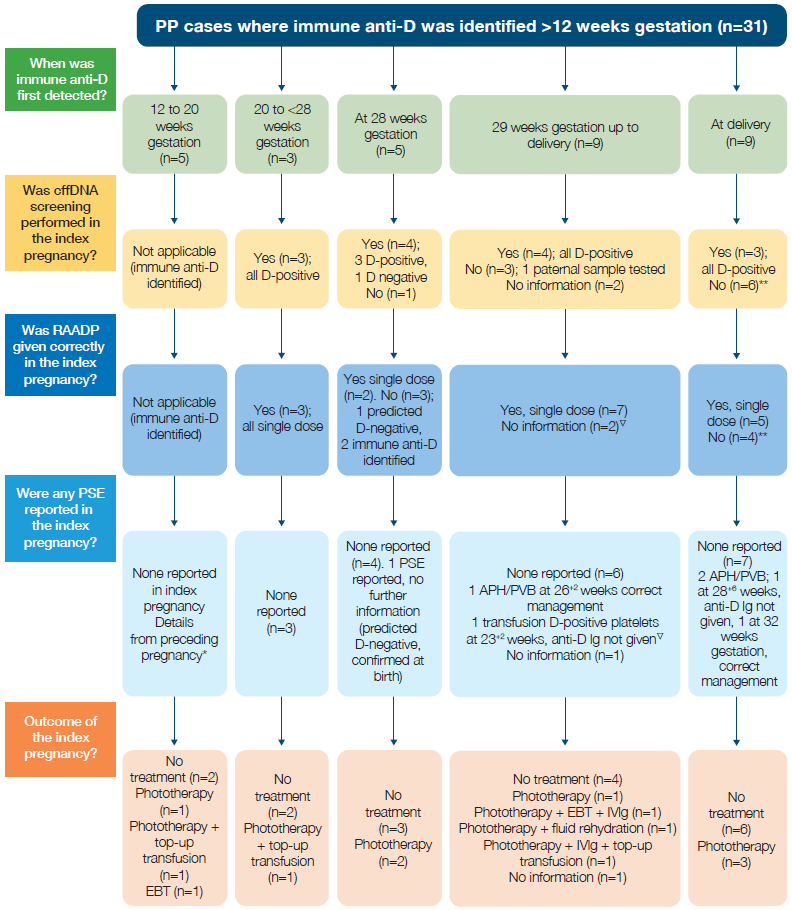
*1 case woman declined prophylaxis during pregnancy and at birth; 1 case previous 3 TOP, in the last TOP no G&S sample taken or anti-D Ig given; 1 case no information available regarding previous pregnancy (abroad); 1 case not reported if anti-D Ig was given after birth in preceding pregnancy
**2 women were treated as D-positive throughout pregnancy, D-variant detected at birth (when immune anti-D was identified). In both cases cffDNA screening testing was not offered and RAADP not given
▽1 case the baby was found to be D-negative at birth, 1 immune anti-D developed following transfusion of D-positive platelets. Case described in Chapter 9, Adverse Events Related to Anti-D Immunoglobulin (Ig) Case 9.1
Conclusion
The presence of immune anti-D in pregnancy can have serious consequences for the fetus and newborn. SHOT data indicate that while most pregnancies result in a live birth, many infants require treatment for HDFN, with phototherapy being the most common intervention. Shared-care pathways continue to influence the quality and consistency of maternity care and can introduce safety risks when communication or processes are suboptimal. SHOT will continue to collect and analyse data on D sensitisation to support best practice and highlight areas for improvement.
Although this chapter focuses on care in the perinatal period, improving standard care applies to all stages of life as highlighted by the renewed Women’s Health Strategy in England (Department of Health and Social Care, 2026). This cross‑life plan aims to fix systemic gaps in women’s healthcare by listening to women’s experiences and redesigning services, promising earlier diagnosis, fairer access, better outcomes and wider economic and societal benefits.
Recommended resources
SHOT Bite No. 29: Differences of reporting errors related to anti-D Ig and immune anti-D
Meet the experts webinar – Anti-D immunoglobulin (Ig) errors and immune anti-D
