Authors: Shruthi Narayan and Claire Wroe with input from the SHOT Team and Working
Expert Group members
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
ACE definition
Exceptional transfusion practice by a team or department, that was above and beyond routine
practice and has widespread learning opportunities.
For a more detailed definition see SHOT Definitions
Introduction
The SHOT ACE category continues to highlight how safe, effective, and compassionate transfusion
practice is delivered every day across the United Kingdom (UK). Building on both Safety-I and Safety-II principles, the category recognises not only great improvement actions to situations where things
occasionally go wrong, but also the far more frequent moments when teams demonstrate resilience,
adaptability, and proactive problem solving to ensure that care goes right, even under pressure
(Crossingham, et al., 2023). These insights help us understand the reality of frontline transfusion practice and how staff maintain safety for patients, blood donors, and colleagues.
In keeping with Safety-II thinking, learning from excellence offers a more holistic view of safety across the transfusion system. It facilitates identification of the conditions, behaviours, and system strengths that enable staff to deliver high-quality care, even when faced with operational challenges, high workload, or limited resources. Many improvement opportunities arise from clinical and laboratory teams who experience these demands daily and who see, firsthand, how their actions protect and benefit patients. By sharing these experiences through ACE reports, staff contribute to a richer, more balanced understanding of transfusion safety.
Although SHOT continues to receive high-quality ACE submissions, the overall number remains low.
This indicates that there is still meaningful work to do to increase awareness and engagement with this category. Several factors may contribute to under-reporting. Some staff may not recognise that every day, positive examples of safe practice are just as important as learning from incidents. Others may worry about the potential impact on their organisation’s data, particularly in environments where a strong focus on adverse events can unintentionally reinforce a negativity bias. More broadly, staffing shortages, sustained workload pressures, and limited time can reduce opportunities for reflective practice and reporting. These barriers may also reflect the prevailing safety culture within teams, where excellence is often seen as ‘routine’ rather than something to be actively shared and learned from.
Positive cognitive balance is an important countermeasure to the well-recognised negativity bias in
healthcare which is the natural tendency to focus on errors, risks, and system failures. Positive cognitive balance describes a shift from an exclusively harm‑focused safety mindset toward a more balanced cognitive framing that includes understanding how safe care is achieved under normal conditions, not only how it fails (Montgomery, et al., 2025). By intentionally recognising what has gone well within a process or clinical interaction, even in pressured environments, staff can develop a more accurate and holistic understanding of safety (Plunkett & Plunkett, 2022). In haemovigilance, this means acknowledging examples of safe practice, effective communication, and strong teamwork alongside traditional incident reporting. Embedding positive cognitive balance within ACE submissions supports a healthier learning culture, helping teams notice the behaviours, decisions, and system safeguards that consistently enable safe transfusion practice.
It is important to emphasise that SHOT ACE is not intended solely for exceptional or rare achievements. The category celebrates the small but significant moments that strengthen transfusion safety: clear communication, shared decision-making, timely escalation, pragmatic problem-solving, and compassionate interactions that make a positive difference to patient experience. These everyday examples help illuminate the strengths of teams and systems, and they offer transferable lessons that benefit the wider community.
This year also marks an important development, as reporting has now been extended to include
colleagues working in the UK Blood Services. SHOT look forward to receiving ACE submissions from
these teams and learning from their expertise, commitment, and the innovative ways they uphold donor and component safety.
The SHOT team would like to acknowledge the professionalism, dedication, and resilience shown by
transfusion staff throughout the UK. The work undertaken by all staff is often carried out under significant operational pressure, but continues to protect patients, support blood donors, and strengthen the entire transfusion pathway. This chapter is intended to recognise, celebrate, and learn from those ongoing efforts.
ACE cases in 2025
A total of 6 cases were submitted: 4 examples of excellence and 2 focused on learning from everyday
events. Although the numbers are small, they still provide valuable insight into current practice, behaviours, and system interactions.
In addition to these submissions, the SHOT team continues to review a wider range of cases from
routine haemovigilance reports, enabling comparison of ACE findings with the broader national picture. This combined analysis will help identify recurring strengths, opportunities for improvement, and areas where targeted support or system change may be beneficial.
The insights from these 6 cases will therefore be considered alongside other SHOT learning to build a
more comprehensive understanding of what supports good practice and where everyday challenges
arise.
Case 5.1: Enhancing patient safety through collaborative standardisation of transfusion requirements
A hospital identified a significant gap in its transfusion pathway: there was no dedicated place or standard process for documenting and communicating specific blood requirements between clinical areas and the laboratory. Information was often buried in digital notes, requiring staff to scroll through multiple entries to confirm whether a treatment or diagnosis had created a new specific requirement. This inconsistency created delays and risked vital information being missed.
In response, the hospital introduced a new specific requirements indicator within the electronic patient record (EPR). This provides a single, clearly visible location for documenting all specific transfusion needs. When the parent clinical team records a new specific requirement, the indicator automatically triggers an email alert to the transfusion practitioner and relevant laboratory managers across the organisation. This ensures the patient’s laboratory information management system (LIMS) record is updated promptly and consistently.
The new system also helps identify incorrect or outdated specific requirements, enabling timely intervention, staff education and reinforcing safe practice. Staff recognised that with this process, communication with external laboratories still relies on the transfusion practitioner contacting them directly. The next planned improvement is to automate this step and address this gap.
Case 5.2: Individual clinical insight leading to improved local transfusion-associated circulatory overload (TACO) risk assessment practice
A staff nurse noticed that a patient with known risk factors for TACO had been prescribed 1037mL of fresh frozen plasma to be infused over 30 minutes. Recognising that this was unsafe, the nurse raised their concerns. This prompted the prescriber to seek advice from the haematology specialist registrar, which led to the transfusion being administered more slowly with prophylactic diuretics.
Although the prescriber had completed a pre-transfusion TACO risk assessment, they had not
identified the same risks that the nurse did. Following this incident, the blood transfusion team updated the electronic pre-transfusion checklist. The previous question, ‘Actions taken to mitigate TACO,’ was replaced with ‘Is the patient at risk of TACO?’ along with clearer response options. When clicked, this question now also displays the SHOT TACO infographic.
This change is designed to support transfusion practitioners and administrators to assess TACO risk themselves and escalate concerns if something has been missed. Every member of staff has a powerful voice and the ability to initiate meaningful change. By fostering a culture that encourages curiosity, questioning, and open dialogue, opportunities are created to identify improvements. Listening to and acting on these insights is key to enhancing patient safety and delivering high‑quality care.
Case 5.3: Improving intravenous administration set storage and packaging to reduce transfusion risk
An initial incident occurred where blood was given through the incorrect giving set. Following the investigation, two contributing factors were identified. First, administration sets in the ward’s clinic drawers had been mixed, resulting in the wrong set being selected. This was recognised immediately and corrected on the ward.
Second, the packaging of the blood administration sets had recently changed. The word ‘transfusion’ had become much smaller, making it difficult to distinguish the blood sets from the standard IV fluid giving sets. The transfusion team were not aware of this change, and the ward had inadvertently mixed the sets while unboxing and storing them, likely caused by the unclear packaging labels.
The manufacturer was contacted, and the safety concerns were escalated. In response, the
packaging was redesigned to clearly identify the set as intended for transfusion, including prominent red labelling to indicate use for blood components. The ward also implemented improved storage practices to prevent giving set mix-ups during re-stocking.
The incident, actions, and key learning points were shared through the Patient Safety Group and cascaded to other wards to reduce the likelihood of recurrence. It is commendable that following a single incident, staff initiated communication with manufacturers and local measures were instituted. Change is most effective when concerns are followed by appropriate actions, including engaging with suppliers and manufacturers. This ensures that any unintended consequences arising from changes to products or processes are identified, addressed, and resolved in a timely manner, ultimately safeguarding both patients and staff.
Case 5.4: Strengthening practice after a missed specific requirement
Following an incident where specific requirements were not met, resulting in an abandoned stem cell harvest, the advanced nurse practitioner (ANP) who identified the issue took steps to improve both their own practice and the wider local system. As a registered non-medical authoriser seeing many transplant patients in follow-up clinics, the ANP now records specific requirements using the dedicated indicator within the EPR. This means staff can immediately view any historic specific requirements.
This entry also triggers a business intelligence alert to the transfusion laboratory. Previously, the laboratory had been unaware of the patient’s irradiated component requirement and stem cell transplant history because their organisation was not involved in the original transplant. The requirement is now recorded on the LIMS to support future transfusion safety.
Use of the specific requirements indicator also allows the transfusion practitioner to vet and
validate the information, notify the appropriate transfusion laboratory if the patient lives outside the hospital area, and check whether any non-irradiated components have been issued. This enables retrospective review, follow-up investigation, and complete incident reporting.
Insights from the ACE cases
This year’s ACE submissions, although small, offer rich insight into what supports safe, reliable transfusion practice. Across the cases, there is clear evidence of how engaged staff, effective digital systems, and strong multidisciplinary collaboration contribute to safer pathways and improved patient outcomes.
Three of the ACE cases demonstrated the impactful role of information technology (IT) solutions and
system integration in strengthening transfusion workflows. Two cases focused on specific requirements, with 1 showcasing an individual driving system-wide improvement and the other highlighting the benefits of coordinated multidisciplinary working. Two of the cases illustrated how digital innovation can streamline processes, reduce error risk, and strengthen overall reliability.
A consistent theme across all cases was the willingness of individuals and teams to step beyond traditional role boundaries, challenge entrenched processes, and influence local and wider system change. This mindset, being inquisitive and recognising where processes can be improved and strengthened, reflects a positive safety culture and a workforce committed to continuous improvement.
Importantly, the themes identified in the ACE cases directly mirror those commonly seen in error reports, but in the opposite direction. Incident reports often highlight problems arising from poor communication, weak teamwork, or ineffective use of IT systems. By contrast, the ACE submissions show strong communication, coordinated teamwork, and effective digital support. The ACE cases therefore complement incident data by showing not only where systems are at risk, but also what enables things to go right.
Figure 5.1: Visualising excellence: word cloud themes from ACE reports (2022–2025)
The ACE ripple effect of acknowledging excellence
Recognising excellence creates a powerful ripple effect across the whole healthcare system. When an
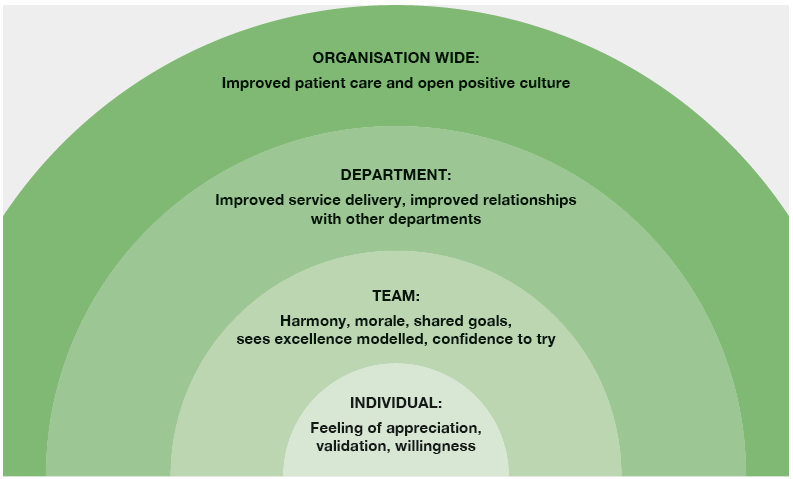
individual feels appreciated and valued, it strengthens their motivation, confidence, and willingness to contribute. This positive experience spreads within their team, fostering better morale, shared goals, and a culture where safe behaviours are modelled and repeated (Birkeli, et al., 2025). At a departmental level, consistent recognition of good practice enhances service delivery, strengthens trust between teams, and supports more collaborative working. As these ripples grow, they influence the organisation, contributing to more open, positive safety cultures where learning is balanced, and psychological safety improves. Ultimately, this has tangible benefits for staff, patients, and blood donors, improving experiences, outcomes, staff engagement, and even joy at work. By celebrating excellence through ACE reporting, organisations strengthen the conditions that allow safe, compassionate transfusion practice to flourish every day (Malone, et al., 2024).
Figure 5.2: Learning from excellence: the ripple effect on practice
How do we learn from ACE events?
Recognising excellence is not only about commending colleagues and teams or celebrating positive
moments. It is also a deliberate learning activity. Excellence events offer rich insights into how safe,
effective practice occurs despite ongoing operational pressures such as staffing constraints, high
workload, or service complexity. By examining how individuals or teams succeeded, valuable insights
into the conditions, decisions, workarounds, and behaviours that made safe transfusion practice possible are gained. These insights can then be shared and replicated across different teams, departments, and care systems, strengthening resilience and supporting more consistent, high-quality outcomes for patients and blood donors. Sharing these examples widely also helps shift the balance away from a solely deficit-focused learning culture, reinforcing the value of noticing what goes well and why. To support this approach, a template document providing guidance on how to optimise learning from excellence events and how to capture these insights meaningfully within SHOT ACE reporting has been developed (see ‘Recommended resources’).
Recognising and reporting examples of excellent transfusion care is just as important as learning from when things go wrong. A SHOT reporter reflected:
SHOT recognising the event as an ACE allows the wider team recognition and is an example of how the actions of a single person or small group can benefit and improve the care for many other patients. Recognising events as ACE ensures that good
practice does not go unnoticed and allows learning to be shared more widely, reinforcing behaviours that improve patient safety and experience.
This view is strongly echoed by the patient perspective. As one patient representative stated:
As a patient, recognising when things go well and actively championing it should be encouraged. We especially as patients are the first to complain albeit informally when things go wrong, yet we don’t credit the staff for all the times where we have had a good experience and care was delivered well.
The same patient representative went on to describe a recent inpatient experience at a hospital where they are not usually transfused.
I was recently an inpatient at a hospital where I am not usually transfused and had to have a unit of blood. The doctor listened regarding my transfusion requirements and had the laboratory call my regular hospital and check and order phenotyped blood in line with my needs. On transfusion, the correct procedures were followed, and I was consented and all the pre-transfusion
checks were done as per protocol. Although this wasn’t reported to ACE as it just followed protocol, for me it was reassurance that away from my usual hospital I felt safe and listened to. I made sure to thank the staff for their professionalism and attentiveness.
Bringing together the perspectives of both SHOT reporters and patient representatives clearly
demonstrates the value of ACE reporting. ACE submissions provide a mechanism to recognise, share
and celebrate these moments of excellence, showing how the actions of individuals or teams can benefit many patients and help embed high-quality transfusion care across the wider system.
Conclusion
This chapter has explored how learning from excellence offers vital insights into what makes transfusion practice safe, resilient, and effective. Despite the high quality of ACE submissions, the overall number of reports remains low; a signal that barriers such as limited awareness, workload pressures, uncertainty about what constitutes ‘reportable’ excellence, and persistent negativity bias may still prevent staff from sharing positive events.
By encouraging reporting of all beneficial practices, not just when things go wrong, ACE supports a
more balanced safety culture where staff understand the value of recognising everyday strengths. For
this to succeed, teams must see clear benefits from reporting and feel confident that good practice is
worth capturing and celebrating. The cases presented this year demonstrate how thoughtful clinical
insight, proactive problem‑solving, and well‑designed digital systems can prevent harm and strengthen transfusion pathways.
Learning from excellence not only highlights what enables care to go right, but also reinforces behaviours and conditions that support safe, compassionate transfusion practice. As safety culture continues to evolve, ACE reporting provides an essential mechanism for sharing practical, real‑world insights that uplift staff, improve systems, and enhance patient and donor safety across the UK.
Recommended resources
Acknowledging Continuing Excellence (ACE) reporting
Optimising Learning from ACE
