Main authors: Dr Lauren Kirkpatrick, Consultant in Transfusion Medicine, Northern
Ireland Blood Transfusion Service (NIBTS), and Dr Asma Sadiq, Specialty Doctor,
NIBTS
With contributions from the Donor haemovigilance chapter writing group comprising:
Dr Shruthi Narayan, SHOT Medical Director and Consultant Donor Medicine, National Health Service
Blood and Transplant (NHSBT)
Dr Liezl Gaum, Specialty Doctor, NHSBT
Robert McGuinness, Lead Specialist Nurse, Clinical Support Team, NHSBT
Georgina Burridge, Lead Specialist Nurse, Clinical Support Team, NHSBT
Dr Jayne Hughes, Specialist in Transfusion Medicine, Scottish National Blood Transfusion Service
(SNBTS)
Dr Champa Manchanayake, Specialty Doctor, SNBTS
Dr Hasarika Dodampegamage, Specialist in Transfusion Medicine, Welsh Blood Service (WBS)
Julie Gardner, Interim Head of Nursing, WBS
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
Definitions
Donor haemovigilance definition
The systematic monitoring of adverse reactions and incidents in the whole chain of blood donor care, with a view to improving quality and safety for blood donors.
Serious adverse reaction: An unintended response in a donor or in a patient associated with the collection or transfusion of blood or blood components that is fatal, life threatening, disabling, incapacitating, or which results in, or prolongs, hospitalisation or morbidity (according to Article 3 (h) of Directive 2002/98/EC).
Recommendation
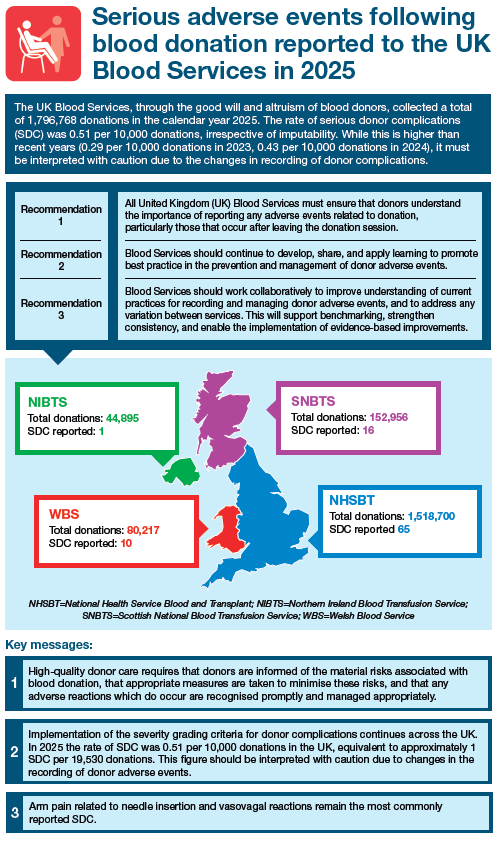
- All United Kingdom (UK) Blood Services must ensure that donors understand the importance of reporting any adverse events related to donation, particularly those that can occur after leaving the donation session.
- Blood Services should continue to develop, share, and apply learning to promote best practice in the prevention and management of donor adverse events.
- Blood Services should work collaboratively to improve understanding of current practices for recording and managing donor adverse events, and to address any variation between services. This will support benchmarking, strengthen consistency, and enable the implementation of evidence-based improvements.
Key messages
- High-quality donor care requires that donors are informed of the material risks associated with blood donation, and that appropriate measures are taken to minimise these risks. Any adverse reactions that do occur should be recognised promptly and managed appropriately.
- Implementation of the severity grading criteria for donor complication continues across the UK. In 2025, the rate of serious donor complications (SDC) was 0.51 per 10,000 donations in the UK, equivalent to approximately one SDC per 19,530 donations. This figure should be interpreted with caution due to changes in the recording of donor adverse events.
- Arm pain related to needle insertion and vasovagal reactions remain the most commonly reported SDC.
Introduction
The UK Blood Services depend on the goodwill and altruism of blood donors to maintain an adequate supply of blood components for patients within the National Health Service (NHS). A safe, sufficient, and reliable blood supply requires a stable base of regular donors who willingly give their time and donate repeatedly. It is therefore essential that Blood Services take all reasonable steps to support the recruitment of new donors and encourage the continued return of existing donors.
European legislation (European Blood Directives 2002/98/EC and 2005/61/EC), subsequently transposed into UK law through the Blood Safety and Quality Regulations 2005 (Department of Health, 2005), requires that donors are informed of the risks associated with donation and that robust governance processes are in place to identify and mitigate those risks. Donor safety is paramount and is upheld through clear donor selection guidelines, standardised policies and procedures, appropriately trained staff, and suitable facilities.
This chapter presents data from the four UK Blood Services on SDC, defined as donor adverse events
graded at grade 3 or above using the severity grading tool. The chapter also includes illustrative cases
and sets out recommendations to support donor care and safety.
Implementation of severity grading of all blood donor adverse events (DAE)
All UK Blood Services record DAE according to the categories outlined in the ‘Standard for Surveillance of Complications Related to Blood Donation’ (Goldman, et al., 2016). The UK Blood Services have been implementing severity grading of donor adverse events following the release of validated donor severity grading criteria. These were developed by the Association for the Advancement of Blood & Biotherapies (AABB) Donor Haemovigilance Working Group and subsequently endorsed by the International Society of Blood Transfusion (ISBT), International Haemovigilance Network (IHN) and European Blood Alliance (EBA) (Townsend, et al., 2020). The grading system categorises the severity of donor adverse events from grade 1 to grade 5, broadly corresponding to mild, moderate, severe, life-threatening events, and death. Further details can be found in the Guidelines for the Blood Transfusion Services, Section 5.10: Donor Adverse Events from the Joint UK Blood Transfusion and Tissue Transplantation Services Professional Advisory Committee (JPAC) (see ‘Recommended resources’). Any event of grade 3 or above is reported as a SDC. Once implemented by all UK Blood Services, the reporting of SDC will replace the previous serious adverse event of donation (SAED) categories.
Implementation of the new severity grading system for donor complications began within the WBS in
January 2024. This was followed by the NHSBT in October 2024 and the SNBTS in January 2025. Full
implementation within the NIBTS is planned to align with the introduction of a new computer system
in 2026. In the interim, measures have been in place within NIBTS since January 2025 to ensure that
data is captured for all SDC. This approach supports consistency in the data presented below across
all four UK Blood Services.
Data from 2025
UK donations
A total of 1,796,768 donations were collected by the four UK Blood Services in 2025 (Table 6.1).
This includes whole blood and component donations, as well as plasma donations collected for the
manufacture of medicinal products.
Table 6.1: Cumulative donation data from the four UK Blood Services in 2025
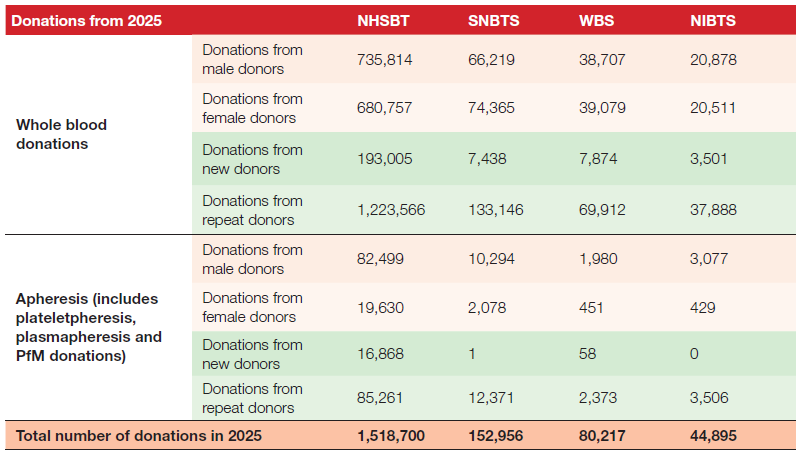
Table 6.2 summarises the number of SDC (grade 3 or above) by category for each of the four UK
Blood Services for the period January 2025 to December 2025. This table includes all cases reported
in 2025 irrespective of the degree of imputability. Arm pain related to needle insertion, 54/92 (58.7%)
and vasovagal reactions, 18/92 (19.6%) continue to be the most frequently reported serious donor
complications. Serious cardiovascular and cerebrovascular events have been reported in temporal
proximity to blood donation, including transient ischaemic attack (TIA), stroke, and myocardial
ischaemia. However, a direct causal relationship with donation cannot be established. Such events
are more likely influenced by donor age and underlying biological risk, with the timing suggesting a
possible temporal association rather than attribution to the donation process itself.
Table 6.2: SDC (grade 3 or above) by category for the four UK Blood Services in 2025
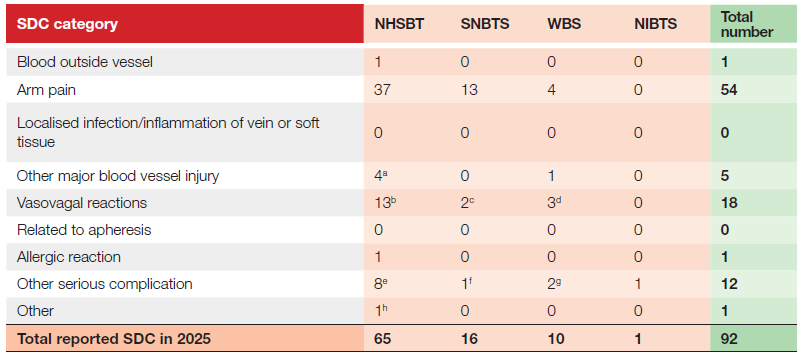
b NHSBT: 9 x vasovagal reactions classified as delayed reactions
c SNBTS: both vasovagal reactions were delayed events requiring hospitalisation
d WBS: 2 x vasovagal reactions classified as delayed reactions
e NHSBT: 1 x acute cardiac symptoms (angina), 4 x cerebrovascular accident (CVA), 3 x TIA
f SNBTS: 1 x TIA
g WBS: 2 x myocardial infarction (MI)
h NHSBT: neuroma in finger following a finger prick 6-7 years ago
Note: data for ‘Arm pain’ SDC is captured in the year the SDC is reported (not necessarily the year in which the event occurred)
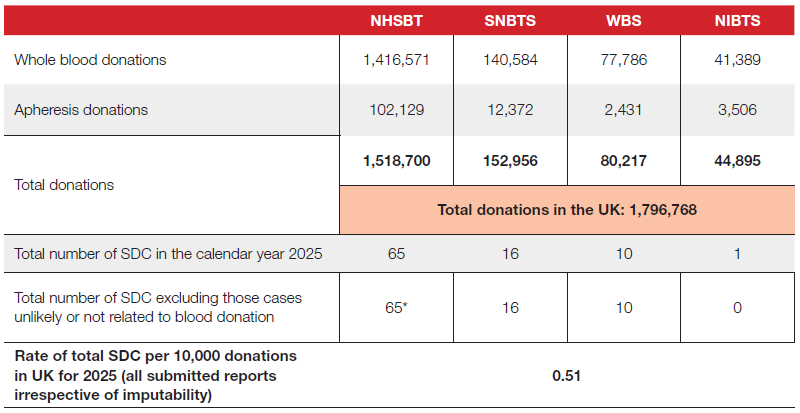
Table 6.3 summarises the total number of donations and SDC reported for each of the four UK Blood
Services in 2025. The rate of SDC was 0.51 per 10,000 donations, irrespective of imputability. While
this is higher than in recent years (0.29 per 10,000 donations in 2023, 0.43 per 10,000 donations in
2024), it must be interpreted with caution due to the changes in recording of donor complications. Most notably, ‘arm pain’ persisting for more than 6 months is recorded as an SDC under the new classification, whereas previously an ‘arm pain’ SAED was defined by a duration of longer than 12 months. It was therefore anticipated that the new grading system would result in more SDC being reported than SAED in previous years. Trends in the subsequent years and the learning from incident investigations and operational insights will inform improvement actions.
It is recognised that there is variation in the rate of SDC reported from each Blood Service. There are
ongoing, multi‑pronged efforts across the UK to better understand existing practices in the recording
and management of adverse events related to blood donation and to address variation, if any, between services. These efforts draw on shared haemovigilance frameworks, collaborative guideline development, standardised definitions, and harmonised reporting systems such as SHOT and SABRE, enabling services to benchmark performance and implement consistent, evidence‑based improvements.
Table 6.3: Summary of total donations for the four UK Blood Services and the total number of
SDC for 2025
Illustrative cases
A small number of illustrative cases are described below. It is important to emphasise that blood donation is generally very safe. The most commonly reported donor complications are mild and include fainting, bruising, and arm pain. The cases discussed here are extremely rare and are presented to promote awareness and highlight learning points, not to discourage donation. These rare events should not deter potential donors from giving blood.
Case 6.1: Myocardial infarction with non-obstructive coronary arteries (MINOCA)
A regular whole blood donor in his 60s donated blood at an afternoon clinic without immediate complications and was discharged feeling well. The following morning, while playing golf, he developed dizziness and malaise that did not resolve with food intake. He subsequently experienced left-sided chest discomfort, shortness of breath, sweating, and a brief episode of impaired consciousness while awaiting ambulance transfer. On hospital admission, electrocardiography demonstrated changes consistent with a non–ST elevation myocardial infarction (NSTEMI), and troponin T levels were markedly elevated. Coronary angiography revealed unobstructed coronary arteries, consistent with MINOCA. Laboratory investigations, including lipid profile, blood glucose, and haemoglobin, were within normal ranges. The patient was managed medically and discharged on oral medications. He was
permanently deferred from further blood donation.
MINOCA is an increasingly recognised clinical entity encompassing heterogeneous pathophysiological mechanisms (Tognola, et al., 2025); however, it is an extremely rare complication following blood donation, with only isolated cases reported in the literature (Şener, et al., 2025). Although adverse reactions following blood donation are usually benign, acute intravascular volume loss and sudden haemodynamic changes may contribute to myocardial injury in susceptible individuals.
This case highlights the importance of careful donor selection and clinical vigilance when blood donors present with post-donation symptoms such as dizziness, hypotension, or chest discomfort, and underscores the need for prompt and comprehensive evaluation in such presentations.
Case 6.2: Upper-extremity deep venous thrombosis (DVT) following blood donation
A regular whole blood donor in his mid-50s presented with progressive swelling of his left arm one week after blood donation. There were no immediate post-donation complications, bruising, or pain at the venepuncture site. Initial assessment by his general practitioner led to treatment with oral antibiotics for suspected infection; however, symptoms worsened, with swelling extending to the shoulder, prompting hospital referral. Investigations demonstrated elevated D-dimer levels, while thrombophilia screening was negative. Doppler ultrasonography confirmed an upper-extremity DVT involving a proximal vein of the phlebotomy arm. The donor was commenced on anticoagulation therapy, with follow-up imaging arranged. Subsequent follow-up confirmed complete clinical recovery. The donor was permanently deferred from further blood donation, as the DVT was considered related to venous cannulation and involved a proximal deep vein.
Upper-extremity DVT is an uncommon but potentially serious condition with a risk of life-threatening
complications, including pulmonary embolism. Outcomes are generally favourable when prompt diagnosis and treatment are instituted (Abidoye, et al., 2025). Donation-related DVT is an extremely rare complication of whole blood donation and is defined as thrombosis occurring in a deep vein of the phlebotomy arm. Symptoms may include pain, swelling, or bruising, with onset ranging from several hours to days following donation.
While additional thrombosis risk factors, such as oral contraceptive use, have been reported in some cases, donation-related DVT can occur in the absence of identifiable hypercoagulable states (Covin, et al., 2004; Featherstone & Bayliss, 1987; Abidoye, et al., 2025). Management typically involves anticoagulation for a minimum of three months. Awareness that blood donation and venous cannulation may be contributing factors is essential, as early recognition and treatment can prevent further complications and reduce longterm morbidity.
Case 6.3: Traumatic neuroma following finger-prick test for pre-donation haemoglobin
Acknowledgements: Claire Griffiths, Clinical Support Team, NHSBT
A regular whole blood donor in her 30s with no significant medical history reported long‑standing pain in her left middle finger, which she believed started after a pre‑donation haemoglobin finger‑prick test. She described years of intermittent but severe fingertip pain with no visible swelling or redness, despite multiple general practitioner (GP) visits for the same issue. The symptoms affected her work as a nurse and worsened after the birth of her child, contributing to low mood. The pain ranged from a constant dull ache to sudden, intense episodes triggered by light touch, sometimes leaving her feeling faint. Her distress eventually led to referrals for further assessment. An ultrasound was normal, but magnetic resonance imaging (MRI) indicated a possible neuroma. A hand specialist advised surgery and agreed
that the finger‑prick procedure was the likely cause, noting this as a rare complication. Surgery later confirmed a glomus tumour, which was removed. At follow‑up, the donor remained pain‑free.
Glomus tumours (and traumatic neuromas which are similar) are reported in the literature as extremely rare (Saba, et al., 2021; Kahraman, et al., 2005). Glomus tumours are generally considered to be benign, but malignancy has been reported on extremely rare occasions (Lee, et al., 2023). They contain regular smooth muscle cells and specialised smooth muscles cells known as glomus cells (Samaniego, et al., 2009). These structures are further surrounded by nerve endings and mast cells that play a role in pain perception. Saba, et al., 2021 report these tumours are more common in females and often misdiagnosed. This can lead to patients experiencing symptoms for many years as was the case in this donor. MRI is considered to be an important diagnostic tool in recognition of these tumours.
This case demonstrates an extremely rare complication of donation. No other cases have been reported to the UK Blood Services in the last five years. Although this is an extremely rare case, there could be under-reporting due to the difficulty of diagnosing such tumours. This case is presented to raise awareness of the possibility that this may need excluding if donors present with pain in their finger post haemoglobin finger prick with a lancet.
Case 6.4: Anaphylaxis in a whole blood donor
A whole blood donor experienced anaphylaxis 10–20 minutes after completing their second donation. The donation itself was uneventful, but shortly afterwards the donor reported light‑headedness and blurred vision, followed by itching, redness, blotching and throat tightness. During post‑donation care, they disclosed a history of severe anaphylaxis to multiple allergens that had not been declared during screening. Session staff immediately called an ambulance while the donor self‑administered two EpiPens. They were transferred to hospital, admitted for several days, and later discharged; latex allergy testing was negative, and no session‑related allergen was identified. Chlorhexidine product details were recorded as a precaution. Staff were able to respond effectively due to recent basic life support and
anaphylaxis‑response training. The donor was permanently deferred from future donations.
Anaphylaxis is a rapid, life‑threatening allergic reaction affecting the airway, breathing or circulation, and may include skin or mucosal symptoms, though these are absent in up to 20% of cases. Common triggers include foods, medications and venoms, and individuals may be unaware of a potential reaction until re‑exposure (NICE, 2020). Donors with a history of allergies or anaphylaxis may donate if symptom‑free on the day and not exposed to known allergens (JPAC, 2022). Donation‑related anaphylaxis is extremely rare, estimated at around 1 in 1 million donations.
Overall, although consent materials, safety checks and supplementary screening aim to minimise risk, donation‑related anaphylaxis cannot be fully eliminated. The process depends on donor disclosure and only identifies known allergens; undeclared, unknown, or indirect exposures, including those introduced by other donors, may still result in an unexpected reaction.
Conclusion
For most donors, the donation process is straightforward and without complication. However, as with any clinical procedure, blood donation carries some risk. Most adverse events are minor and resolve quickly, but serious adverse events, although rare, may have potentially lifelong consequences for the donor. Even minor complications can negatively affect the donor experience and impact donor retention. It is therefore essential that the prevention of adverse events remains a priority and that, when donor complications do occur, they are recognised promptly and managed appropriately.
All donors must receive clear post-donation information. Blood Services should ensure that donors
understand the importance of reporting any adverse events of donation, particularly those that arise after leaving the donation session. Donors should be encouraged to make early contact with the Blood Services team so that timely investigation and management can be undertaken. Continued surveillance, improved understanding of complications and associated risk factors, and systematic learning from reported events will support ongoing improvements in the quality and safety of the donor experience.
Recommended resources
Donor Haemovigilance Hub: resources related to donor haemovigilance, especially donor
care and safety