Authors: Clare Cook, Jennifer Davies and Vera Rosa
Link to PDF chapter Link to supplementary information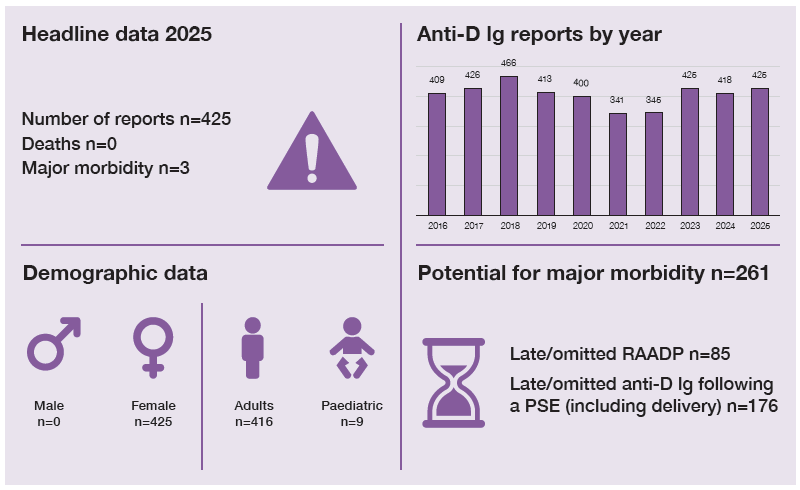
Key SHOT messages
Key findings
- Omission or late administration remain the main causes of anti-D Ig errors.
- Information technology (IT) was a factor in almost 25% of cases.
- Omission of anti-D Ig after transfusion of D-positive components to D-negative women/birthing people of childbearing potential persists.
Gaps identified
- Discrepancies in national guidance for anti-D Ig use in early pregnancy.
- Lack of awareness that management of potentially sensitising events (PSE) and routine antenatal anti-D Ig prophylaxis (RAADP) should be treated as separate events.
- Discrepant cell-free fetal deoxyribonucleic acid (cffDNA) results may be under-reported to SHOT.
Good practice
- Reports showed improved practice through corrective and preventive actions (CAPA).
- Use of structured communication tools (e.g. SBAR – situation, background, assessment,
recommendation), verbal handover, and dedicated data fields in electronic patient records (EPR) and paper records.
Next steps
- A national comparative audit (NCA) in April–June 2026 identified practice gaps; findings (due October 2026) should inform review of local policies and processes.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Adverse Events Related to Anti-D Immunoglobulin (Ig) definition
Events relating to the requesting and/or administration of anti-D Ig and RAADP during pregnancy and after delivery.
For a more detailed definition see SHOT Definitions
Introduction
Timely and correct administration of anti-D Ig to D-negative people of childbearing potential (including paediatric) is crucial to prevent D sensitisation. During pregnancy, anti-D Ig should be given following every PSE, including birth, and as part of RAADP (Qureshi, et al., 2014). Prenatal non-invasive screening for RHD supports targeted anti-D Ig administration, avoiding unnecessary use where the fetus is predicted to be D-negative. Anti-D Ig is also required when D-negative people of childbearing potential are transfused with D-positive blood components or are recipients of a D-mismatched solid organ transplant (Austin, et al., 2009; Qureshi, et al., 2014).
Errors occur at every step of the transfusion pathway, highlighting the complexities of anti-D Ig
management. In 2024, SHOT published an anti-D Ig safety notice and a gap analysis, both available on the SHOT website (see ‘Recommended resources’). The NCA for anti-D Ig use in pregnancy took place between April and June 2026 and the report is planned to be published at the end of October 2026. It aims to identify variation in local processes and support hospitals in strengthening their pathways (NHSBT, 2026).
Major morbidity n=3
Three cases resulted in major morbidity (sensitisation to the D antigen). Two were due to failure to
administer RAADP; in one case RAADP was not given as a dose had been recently administered to
cover a PSE. In both cases, immune anti-D was identified at birth. In the third case, anti-D Ig was not
given following a transfusion with D-positive platelets during a major haemorrhage (MH) that occurred during pregnancy (Case 9.1).
Case 9.1: Transfusion of D-positive platelets in pregnancy during MH
A 23-week pregnant patient with multiple comorbidities attended the emergency department with a gastrointestinal bleed requiring urgent transfer to theatre. The MH protocol was activated, and the transfusion of D-positive platelets was approved by the haematology consultant. Anti-D Ig was not requested by the clinicians and consequently its administration was omitted. Immune anti-D was detected later in pregnancy. No impact upon the baby was reported.
The review of the case identified a knowledge gap in the clinical team, who were unaware of the requirement for anti-D Ig following a transfusion of D-positive blood components to D-negative patients of childbearing potential. Cognitive bias also impacted the event as the clinicians were focused on managing the bleed and stabilising the patient. Improvement in communication from the laboratory to the clinical team when anti-D Ig is required has been highlighted as an action.
Overview of anti-D Ig error cases reported in 2025 n=425
A total of 425 cases were analysed: 150 related to PSE in pregnancy, 152 to RAADP and 120 following
birth. Additionally, 3 cases were related to non-pregnant women of childbearing potential. Four cases
involved transfusion of D-positive blood components (1 red cells, 3 platelets). The amber alerts issued by the national Blood Services, related to stock shortages, were noted as a contributory factor in 2 cases.
Figure 9.1: Distribution of anti-D immunoglobulin (Ig) related errors reported in 2025 (n=425)
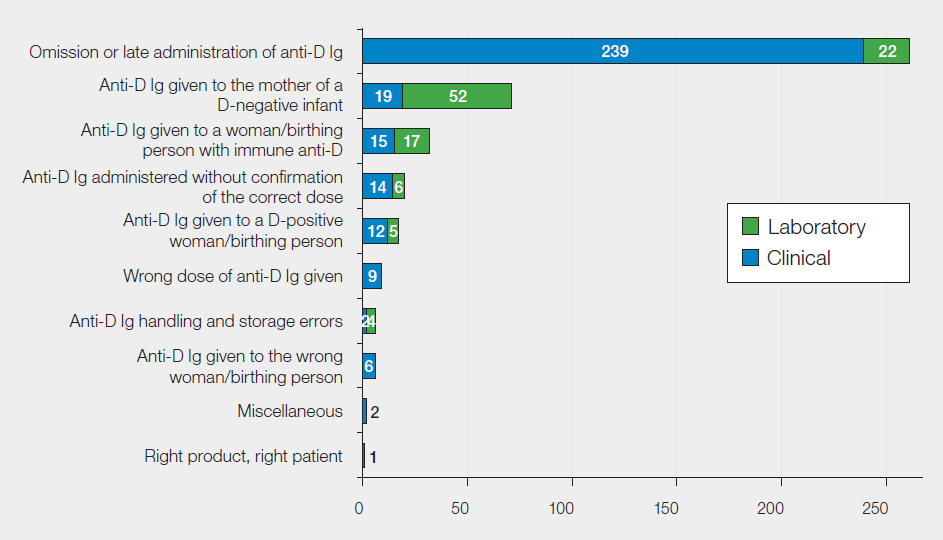
There were 319/425 (75.1%) reports related to errors in clinical settings and 106/425 (24.9%) in the
laboratory. As in previous Annual SHOT Reports, most events resulted in omission or late administration of anti-D Ig, 261/425 (61.4%); and these are further broken down in Table 9.1.
Table 9.1: Causes of omission or late administration of anti-D Ig in 2025 (n=261)
| Reason for omission or late administration | Number of reports | Percentages of cases |
| Anti-D Ig not ordered | 76 | 29.1% |
| Discharged before anti-D Ig administration | 54 | 20.7% |
| Anti-D Ig ordered but not administered | 32 | 12.3% |
| Incorrect decision to omit anti-D Ig administration | 27 | 10.3% |
| Maternal or neonatal results not checked or misinterpreted (not related to cffDNA) | 18 | 6.9% |
| D variant women/birthing people | 16 | 6.1% |
| Errors related to cffDNA (test and results) | 16 | 6.1% |
| Transcription errors (not related to cffDNA) | 14 | 5.4% |
| Deviation from laboratory processes (not related to cffDNA) | 6 | 2.3% |
| Positive patient identification (PPID) not carried out at sample taking | 2 | 0.8% |
| Total | 261 | 100% |
Discrepancies in national guidelines continue to contribute to anti-D Ig errors in early pregnancy which has been highlighted in the supplementary information for this chapter.
Non-invasive prenatal screening for RHD (cffDNA) n=76
In 2025, 76 cffDNA screening-related events were reported to SHOT. Errors occurred at all steps of the
transfusion pathway with higher representation at request, 18/76 (23.7%), and testing, 47/76 (61.8%).
The causes of the events are further broken down in Figure 9.3, in the supplementary information.
Laboratory cases related to cffDNA screening results n=51
Screening testing for fetal RHD is available across the UK for non-immunised D-negative pregnant people, as recommended by the National Institute for Health and Care Excellence (NICE, 2016). Currently there are three test providers in the UK and this test now has an uptake of 88% in England (as of November 2025). The limitations of the screening assay are known with a sensitivity of 99.3% (95% confidence interval (CI) 0.982-0.997) and a specificity of 98.4% (95% CI 0.964-0.993) (Mackie, et al., 2017). In 2025, 46 cffDNA false-positive and 12 false-negative results were reported to the test providers. This suggests under-reporting to SHOT, as 38 false-positive and 7 false-negative cffDNA events were reported to SHOT in the same year.
The remaining 6 laboratory cases involved incorrect or missed result checks, 5 of which led to unnecessary anti-D Ig administration.
Clinical cases related to cffDNA screening results n=25
There were 25 clinical cases related to cffDNA screening results; 17 led to unnecessary use of anti-D Ig
and 8 to omission/late administration. The main cause of unnecessary administrations was omitting to review the cffDNA result. Contributory factors included assumptions that other staff had performed the result review and acting on unconfirmed information. IT systems were noted as contributory to the event in 4 cases, including unused or unheeded flags in the system and lack of awareness of where to check the results. Insufficient computers and the need to use multiple systems has been reported as a concern. Knowledge gaps relating to local policies and the recent implementation of the test were also reported.
Of the 8 cases of omission/late administration, 7 were related to RAADP and 1 following birth. In most of the RAADP cases (5/7), not reviewing the cffDNA result led to pregnant people not being placed on the correct care pathway for their pregnancy. In the remaining 2 cases, the cffDNA result reviewed was from a previous pregnancy and in one of these cases the pregnancy was related to a different birthing person.

Involvement of information technology (IT) n=105
Figure 9.2: The impact of information technology in anti-D Ig errors (n=105)
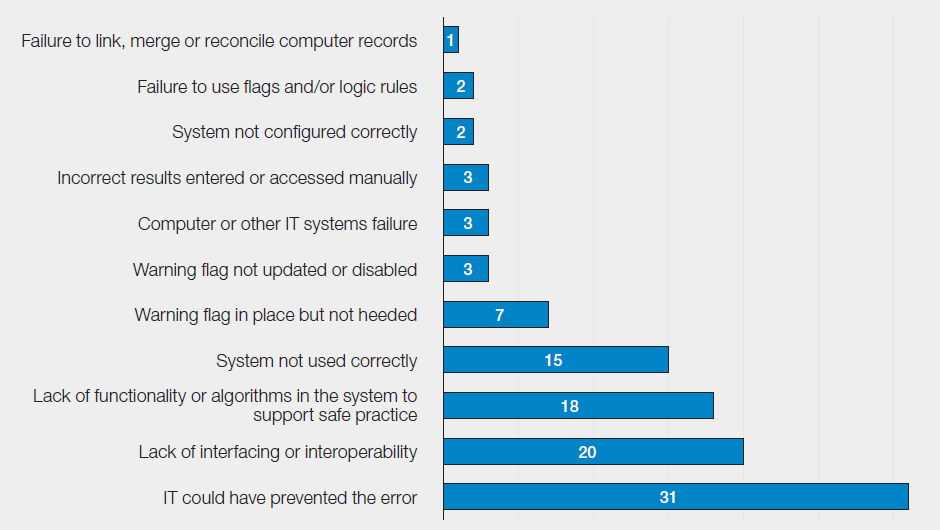
IT systems were recognised as a contributory factor in 74/425 (17.4%) cases and in 31/425 (7.3%)
cases as a potential preventive measure (Figure 9.2). Further breakdown of the IT impact is available in the supplementary information on the SHOT website. SHOT has previously highlighted that manually inputting data poses a risk for patient safety, as discussed in the Problem Statement issued in August 2024 (see ‘Recommended resources’).
Shared care n=67 and handover n=84
Pregnancy care is often shared between multiple teams, which can be within a hospital, between local hospitals and the community or across boundaries of different healthcare organisations. Shared care requires a seamless transition of information to minimise opportunities for error.
At an organisational level, clear, formal channels of communication between teams and across borders could have prevented some of the events reported. Assumptions about responsibility for varying aspects of care led to time-sensitive interventions being missed. An absence of service-level agreements between care providers in NHS and private services also led to delays and confusion.
Communication and documentation continue to be contributory factors for anti-D Ig administration
errors, in both shared-care cases and within individual teams. Themes identified included information not being documented, documented but not seen, misinterpreted, use of auto text, copying and pasting incorrect information, and information not handed over.
Handover contributed to errors in 84/425 (19.8%) cases. Of these, 53/84 (63.1%) stated that a structured handover process was in place. This suggests that although structured handovers are used, there are opportunities for improvement.
Case 9.2: Woman with immune anti-D given anti-D Ig
Immune anti-D was detected in a pregnancy after the 28/40 RAADP and care was transferred to the fetal-maternal medicine unit (FMU). Due to gaps in the EPR, the FMU team did not document a plan of care for delivery. Unaware of the immune anti-D status, the delivery team requested a kleihauer and anti-D Ig, which was declined by the laboratory. A haematology registrar supporting the laboratory was unable to access clinical information from the Blood Services, which showed increasing antibody titres. Based on the information available at the time, the haematologist supported the request for anti-D Ig, resulting in an inappropriate administration. No adverse effect on the baby was reported.
As a result of learning from this case, the digital team planned to create a dedicated care/communication plan in the EPR.
Near miss (NM) anti-D Ig cases n=19
There were 19 cases of NM anti-D Ig analysed in 2025, a decrease from 2024 (n=40) and 2023 (n=41).
Most errors were identified at administration, 10/19, or during review of results by the clinical team,
4/19. The remaining 5 cases were detected by the laboratory either at sample testing, results checking, routine equipment checks or when anti-D Ig was returned to the laboratory.
Learning points
- Interoperability between different IT systems in the laboratory and clinical settings can prevent transcription errors and misinterpretation from occurring.
- Safe, timely and effective communication can reduce the risk of error. The use of frameworks and tools such as SBAR, I-PASS (illness severity, patient summary, action list, situation awareness and contingency planning, synthesis by receiver) and closed loop communication supports clarity and understanding. Organisational support includes providing appropriate facilities and an environment that is sensitive to the effect of human factors on communication.
Conclusion
Errors related to the use of anti-D Ig continue to account for a significant number of cases reported to
SHOT each year, with omitted or late administration comprising the largest sub-category. Errors occur
at every step in the transfusion pathway, with significantly more occurring in clinical settings as opposed to the laboratory. The SHOT Safety Notice released in 2024 aimed to raise awareness and signpost healthcare providers to resources to support safe practice. Teams are encouraged to use these resources and work collaboratively to identify gaps in practice and opportunities for improvement, across all settings.
An increase in the use of technology has allowed more targeted use of anti-D Ig, with non-invasive
pre-natal testing of fetal RHD widely available to the majority of healthcare organisations in the UK.
However, this has created further opportunities for error to occur. As the use of EPR systems increases, organisations should look to harness their functionality to improve the management of anti-D Ig. Further guidance on how IT systems can support the appropriate administration of anti-D Ig can be found in the recommended resources.
Recommended resources
Anti-D Immunoglobulin (Ig) Errors Cumulative Data
