Authors: Caryn Hughes, Nicola Swarbrick, and Victoria Tuckley
Link to PDF chapter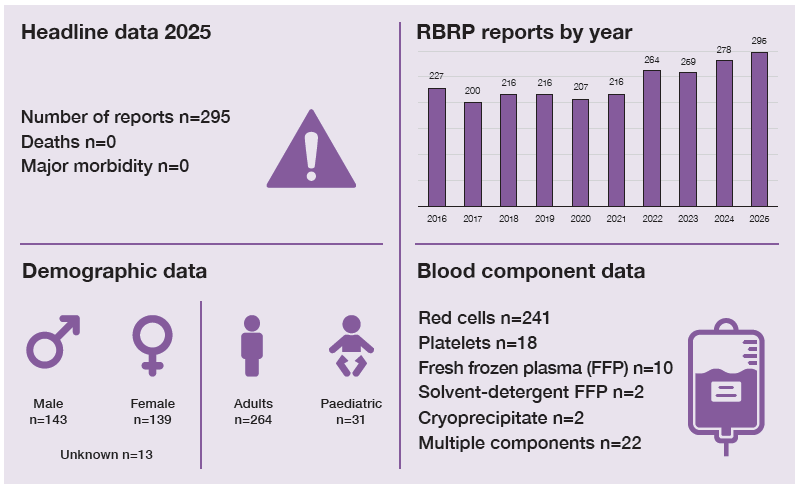
Key SHOT messages
Key findings
- Clinical RBRP errors have increased in 2025.
- Prescription/authorisation errors increased, including transfusions without written authorisation.
- More laboratory RBRP errors involved information technology (IT)-related contributory factors.
- Overall near miss (NM) RBRP cases decreased by more than half; however, clinical NM cases doubled compared with 2024.
Gaps identified
- Accurate patient identification (PID) is not consistently performed at critical points.
- Pre-transfusion checklists completed as a formality rather than used as an active safety measure.
- Limited laboratory IT system functionality, including lack of algorithms and interoperability.
Good practice
- Human factors principles were applied during most incident investigations of RBRP cases.
- In NM RBRP, more than half of errors were detected at the pre-administration checking process, with most using a formal pre-administration checklist.
Next steps
- Regular audits of pre-transfusion checklist use, including the authorisation of blood components, can help identify potential errors and highlight opportunities for improvement.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
RBRP definition
Incidents where a patient was transfused correctly despite one or more serious identification (ID) or prescription/authorisation errors which in other circumstances might have led to an incorrect blood component transfused (IBCT).
For a more detailed definition see https://www.shotuk.org/reporting/incident/definitions/
Introduction
There were 295 cases reported in 2025, an increase from 2024 (n=278). Clinical cases accounted for
235/295 (79.7%) and laboratory cases 60/295 (20.3%). Clinical cases increased from 74.1% in 2024,
and laboratory cases decreased from 25.9%.
Deaths and major morbidity related to transfusion n=0
There were no deaths or major morbidity related to the transfusion as a result of RBRP errors.
Overview of RBRP errors
Primary RBRP errors occurred across nine of the ten transfusion process steps. Patient demographic
inaccuracies in both clinical and laboratory settings accounted for 148/295 (50.2%) of cases. PID errors occurred throughout the transfusion process, with 92/148 (62.2%) arising from errors with labelling of samples and request forms in clinical areas. Laboratory-related PID errors accounted for 29/148 (19.6%), primarily due to incorrect data selection or entry into the laboratory information management system (LIMS), failures in record linking or reconciliation and identification data not being properly checked.
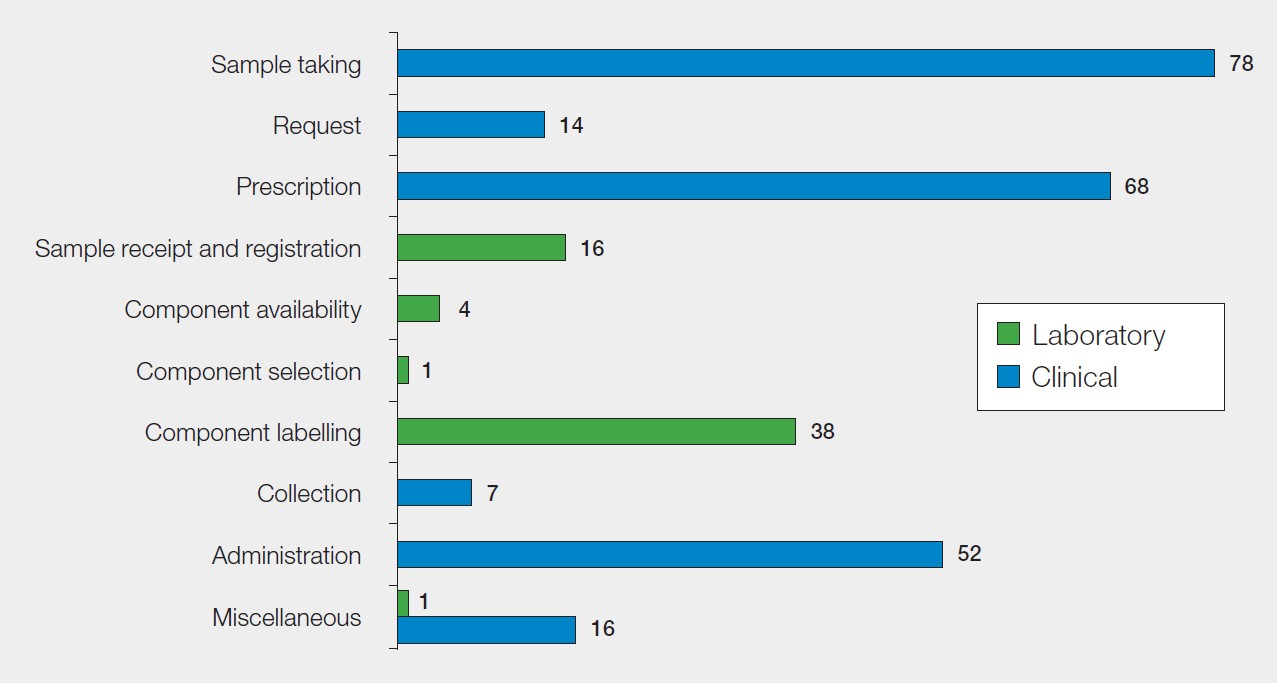
Figure 17.1: RBRP classified by the step in the transfusion process where the primary error
occurred in 2025 (n=295)
Clinical RBRP errors n=235
The highest number of errors in clinical RBRP occurred at sample taking, 78/235 (33.2%), followed
by prescription/authorisation errors, 68/235 (28.9%) (Figure 17.1). Administration errors accounted for 52/235 (22.1%) of cases, including 11 instances where patients were transfused without a wristband and six where PID errors were missed.
A substantial proportion of reports were associated with PID errors, 119/235 (50.6%), and IT contributed to errors in 155/235 (66.0%) of cases. Most IT-related errors were attributed to inadequate system functionality, selection of incorrect patient details, or incorrect use of the IT system. In 85/155 (54.8%) of reports, the use of IT could have prevented the error.
Case 17.1: Blood component administered without patients details on the authorisation chart
An obstetric patient undergoing a planned caesarean section, received one unit of red blood cells as a top-up transfusion without PID details being documented on the blood authorisation chart. No care plan was evident in the patient’s notes and there was no evidence that pre-transfusion safety checks were carried out. The blood transfusion authorisation documentation was frequently attached to the drug chart, and it was noted, after discussion with the staff members, that they had used the drug prescription chart to check the patient’s identification details. This contradicted hospital policy which was to complete PID on both sets of documentation.
Following local investigation, contributory factors identified were the absence of an IT system due to funding constraints, and communication issues between the staff members involved in administering the transfusion. The situation was exacerbated by the patient being transferred to a different ward for the transfusion. Not using a pre-transfusion safety checklist resulted in a missed opportunity to detect the error prior to commencing the transfusion.
Prescription/authorisation errors n=68
Of the 235 clinical errors, 68/235 (28.9%) were related to prescription/authorisation errors. Of these,
41/68 (60.3%) patients were transfused without documented authorisation. IT, including electronic
patient records, was implicated in 35/68 (51.5%) events. These included 27 cases where IT could
have prevented the error, 6 events where IT systems were not used correctly and 2 cases where a lack
of functionality or algorithms in the IT system to support safe practice contributed to the error. A pretransfusion checklist had been used in 43/68 (63.2%) but failed to detect the error.
Pre-administration checklists
A pre-administration safety checklist was used in 146/235 (62.1%) of all clinical RBRP cases but failed
to detect the error. In 78/235 (33.2%) it was stated that a checklist was either not used, not available
or not applicable. In 11 cases, no information was provided.
Learning points
- Pre‑transfusion checklists are a key safety tool to support accurate patient identification, appropriate authorisation, and correct blood component compatibility.
- Written authorisation of blood components is a legal requirement to ensure safe transfusion practice and regulatory compliance (Department of Health, 2005).
Laboratory RBRP errors n=60
Component labelling errors n=38
Blood component labelling errors accounted for 38/60 (63.3%) of laboratory RBRP errors. Labelling
errors due to transposition of labels between blood components intended for the same patient accounted for 22/38 (57.9%). Seven cases involved incorrect patient demographics on compatibility labels and in 7 cases blood components were issued and transfused without required labels, including traceability, emergency, or patient identification. In the remaining cases, no further details regarding the labelling errors were available.
Sample receipt and registration (SRR) errors n=16
All SRR errors involved incorrect details on the compatibility label. These errors were largely due to
demographic data entry errors (6/16), available information on the sample or request form not heeded (6/16) and missed information on the request form (4/16). Errors related to the use of IT occurred in 52/60 (86.7%) laboratory RBRP cases. The IT systems most implicated were LIMS, electronic blood management systems, and electronic patient records. Issues included system failures, poor record linkage and reconciliation, selection of incorrect patient details, insufficient system functionality to support safe transfusion practice, and lack of interoperability.
Case 17.2: Blood component compatibility label mismatch alert unheeded after name change
A name was changed on the patient administration system from ‘Stephen’ to ‘Steven’. The sample and request form contained the new spelling (‘Steven’). The sample was booked in under the older name (‘Stephen’), so the issued component and compatibility label still carried the outdated details. At the bedside, an electronic blood management system was used to administer the component, and a compatibility label mismatch error occurred. The alarm was disregarded; the blood component was manually checked and administered despite the alarm alert and mismatch.
This case highlights gaps in PID processes and lack of appropriate use of IT systems that support safe transfusion. Safe transfusion relies on correct PID and strict pre-transfusion safety checks; bypassing either of these greatly increases the risk of serious error.
Contributory factors to RBRP errors
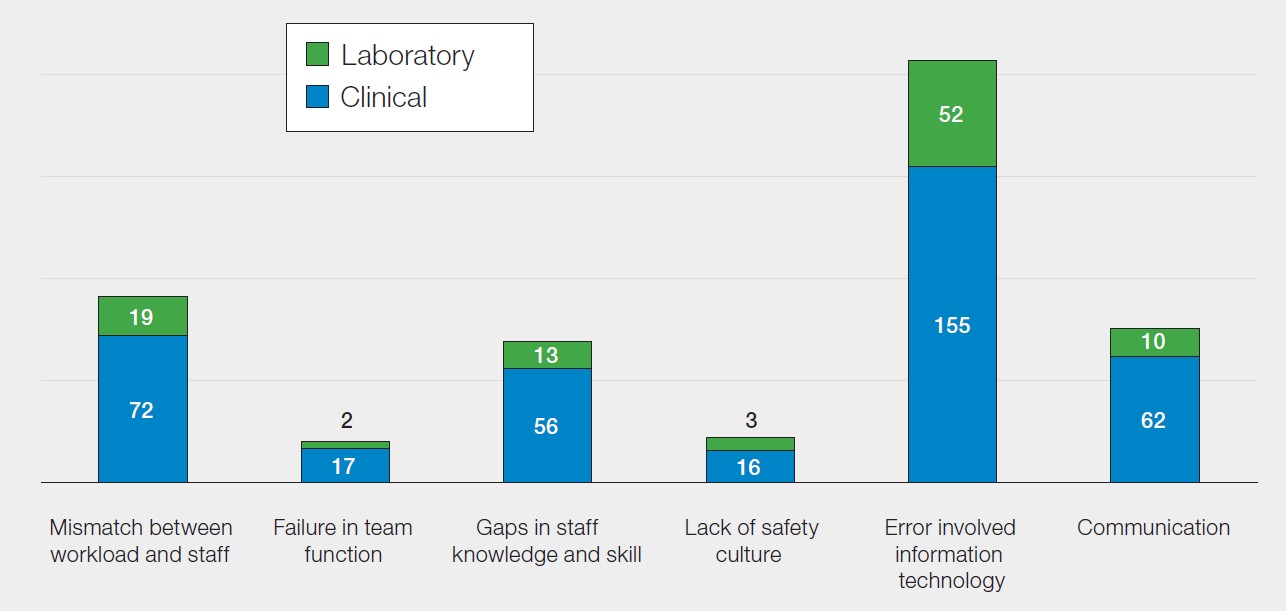
Human factor principles were applied during the investigation of transfusion-related adverse events
in 196/235 (83.4%) clinical cases and 48/60 (80.0%) laboratory cases. Errors with IT featured notably
as a contributing factor in RBRP errors including ineffective system integration, limited functionality or algorithms to support safe practice, incorrect use of systems, and occasional system or equipment
failures. These issues can lead to inaccurate or inconsistent patient information, missed or overridden
alerts, an increased reliance on manual checks, thereby increasing the risk of patient identification,
authorisation, and compatibility errors.
Reviewing contributory factors after an error is essential for preventing recurrence and improving
patient safety. Most healthcare errors are as a result of system and process deficiencies, such as poor
communication, high workload, or inadequate safeguards, rather than individual blame. Analysing these issues supports learning, strengthens safety culture, and guides effective corrective actions (NHSE, 2015).
Figure 17.2: Contributory factors in RBRP errors reported in 2025
NM RBRP cases n=65
There were 65 NM RBRP incidents, 21/65 (32.3%) originated in the clinical area and 44/65 (67.7%) in the laboratory. Component labelling errors, 32/44 (72.7%) accounted for most NM cases in the laboratory. In the clinical area, sampling errors, 10/21 (47.6%) were the most reported. In 44/65 cases (67.7%), errors were detected during the pre-transfusion administration checking process. Of these, 37/44 cases (84.1%) involved the use of a formal checklist.
Conclusion
Pre-administration patient side safety checks can detect RBRP errors, but these must be carried out
correctly to be effective. Blood component labelling issues, particularly the transposition of labels for
the same patient, along with failures in patient identification and missing labels continue to contribute to laboratory errors. The high proportion of IT-related errors highlights significant system limitations, including poor interoperability and inadequate functionality, contributing substantially to transfusion risk. There is a misconception that IT solutions are the only way to prevent RBRP errors, but some reports highlight that, unless they are integrated and used correctly, errors still occur.
Recommended resources
SHOT Video: The Pre-administration Blood Component Transfusion Bedside Check 2020
Safe Transfusion Practice: Transfusion Checklist
SCRIPT Using Information Technology for Safe Transfusion
