Authors: Victoria Tuckley, Nicola Swarbrick, Pete Baker and Heather Clarke
Link to PDF chapter Link to supplementary information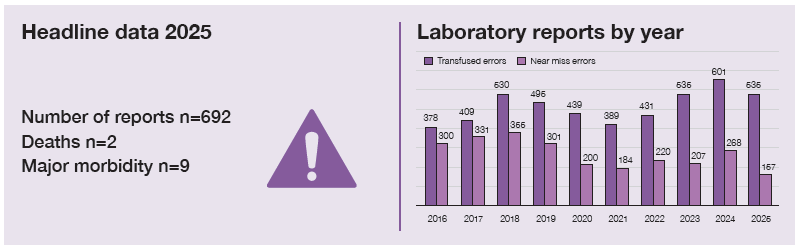
Key SHOT messages
Key findings
- Laboratory errors contributed to 2 patient deaths, both due to delayed transfusions.
- There has been a large increase in major morbidity caused by laboratory errors, with cases more than doubling to 9 in 2025 from 4 in 2024.
- There were 3 cases of ABO-incompatible (ABOi) transfusion of plasma components.
- There was an increase of cases occurring during the component availability step, with the number of errors at other steps decreasing.
Gaps identified
- Delays in transfusion and lack of component availability with profound patient impact.
- Not meeting transfusion requirements for patients of childbearing potential.
- Inadequate capacity planning and staff support systems.
- Insufficient training support for newly qualified transfusion laboratory staff.
- Lack of actions and effectiveness review following investigation.
Good practice
- Duty of candour practice has been followed through relevant communication channels.
- Over 90% of laboratory reports have been reviewed through governance procedures.
Next steps
- Evaluate capacity plans to ensure laboratories are staffed to meet service needs.
- Meaningful changes should be implemented after incident review to prevent reoccurrence.
- Implement and maintain SHOT Safety Standards in the laboratory.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
Introduction
There has been a decrease in laboratory error reports in 2025 to 535 from 601 in 2024, however this
is still higher than the average number of laboratory error reports over the past 10 years (mean n=474). The largest reduction has been seen in the delayed transfusion category which has decreased by approximately a third (82 in 2025 from 120 in 2024). Near miss (NM) reports have also decreased to
157 from 268 in 2024. There were 3 cases of ABOi transfusions caused by a laboratory error in 2025, all
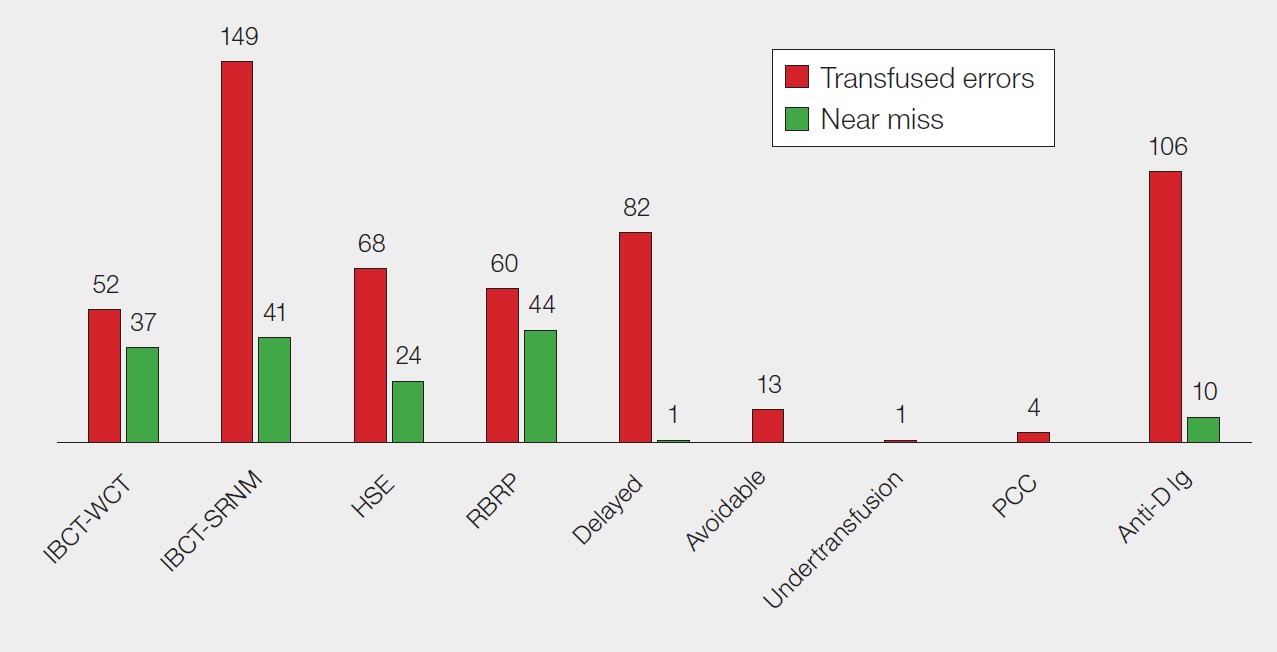
were related to plasma components. The largest number of laboratory error reports related to incorrect blood component transfused-specific requirements not met (IBCT-SRNM), 149/535 (27.9%), followed by anti-D immunoglobulin (Ig) errors 106/535 (19.8%) (Figure 18.1).
Figure 18.1: Laboratory errors and near misses in 2025 (n=692)
A reduction in reports may reflect several possible factors, including a genuine decline in laboratory
errors, reduced detection of errors, or a decreased capacity to participate in haemovigilance. However, because the decrease in error reports is accompanied by fewer NM reports and an increase in cases involving patient harm, it is unlikely that this reduction accurately represents the true number of laboratory-related transfusion incidents.
Deaths related to transfusion n=2
In 2025 there were 2 deaths related to errors within the laboratory. Whilst this is a decrease from the
3 deaths in 2024, this remains a higher rate than expected. Both deaths in 2025 related to delays in
blood transfusion.
One death was probably related to the transfusion (imputability 2) due to a delay in transfusion
compounded by incomplete laboratory handover and communication. This is described as Case 18.1.
The second death was possibly related to the transfusion (imputability 1) due to a delay in provision of fresh frozen plasma (FFP) in a major haemorrhage scenario. A full case description can be found within supplementary material for this chapter.
Case 18.1: Death related to delay in transfusion due to incomplete handover and lack of recognition of clinical urgency (imputability 2 – probable)
A patient with a likely new diagnosis of transfusion-related acute myeloid leukaemia on background of myeloma was admitted to the emergency department (ED) with a haemoglobin (Hb) of 56g/L and platelet count of 8×109/L. They were stable and had been receiving regular top-up transfusions over the past 2 months. Red cells were requested and as the patient had atypical red cell antibodies the sample needed to be tested at the reference laboratory. Clinicians were informed the estimated time of red cell delivery would be on the following day, but the haematology consultant was not contacted for advice by laboratory staff as per policy.
Information about the impending delivery and urgent transfusion was not verbally handed over at laboratory shift change. The units were recorded as being expected on the laboratory handover sheet, but the urgency of the transfusion was not logged. The red cells arrived much quicker than expected, but the ED was not informed that they were available. The clinical team were hesitant to transfuse emergency group O red cells due to the presence of alloantibodies, despite the patient’s Hb dropping further to 40g/L during this period. No further communication was made by the ED team to the laboratory to chase blood availability as they were expecting the delivery the next day. Fifteen hours after admission an emergency call was made as the patient had collapsed onto the floor with cardiac arrest an hour after they had last been reviewed. A unit of emergency O D-positive blood was administered but the patient did not survive.
There was no bed available on the haematology ward, so the patient remained in the ED for the whole 15 hours. The investigation noted the ED was extremely overcrowded with excessive corridor care. It also noted a hesitancy from the clinical teams to use emergency blood due to red cell antibodies being present. Advice was sought from haematologists upon admission, but they were not contacted after this for further guidance despite deterioration.
Learning points
- Clear complete handover of urgent tasks is essential for patient safety.
- For complex cases, input from haematology consultants should be sought initially and for ongoing clinical management.
- Regular patient monitoring is essential to recognise any change in clinical picture.
- Consider using concessionary release pathways to prevent delays in blood provision.
Major morbidity n=9
There were 9 cases of major morbidity attributed to laboratory errors in 2025, which is a large increase from 4 cases in 2024. This year 4 cases were due to laboratory delays in the availability of blood components and 3 cases were due to sensitisation to the D antigen in patients of childbearing potential. The remaining 2 cases were due to sensitisation to the K antigen in patients of childbearing potential. Case 10.9 in Chapter 10, Incorrect Blood Component Transfused (IBCT) describes a case of sensitisation to the K antigen with profound patient impact, and Case 18.2 describes a case of major morbidity due to delayed transfusion. Remaining case descriptions can be found within the supplementary material.
Case 18.2: Delay in blood provision for exchange transfusion causing admission to paediatric intensive care unit (ICU)
A known sickle cell patient was urgently transferred from another hospital to a paediatric high
dependency unit (HDU) with sickle cell crisis at 19:30. The HDU, clinical haematology and blood transfusion laboratory were informed prior to admission of the need for an urgent red cell exchange transfusion. Eight suitable units of red cells were ordered from the Blood Service prior to arrival in readiness.
A sample for crossmatching was taken and sent via the pneumatic tube system at 21:30 to the
pathology specimen reception. The sample did not arrive in the transfusion laboratory until 23:39. Specimen reception staff had no system in place to differentiate routine or urgent samples. Crossmatching was carried out manually as a neonatal sample tube had been used and the volume of blood was insufficient for the analyser, causing further delay.
A discussion took place with the haematology consultant as to whether irradiated red cell components were needed, and the decision was that this was not necessary. The historical local policy in place for paediatric HDU and ICU was that all blood components to these areas should be irradiated. This requirement was set up in the laboratory information management system (LIMS) and the electronic blood management system (EBMS), so the BMS had to override multiple alerts on the system when allocating the red cell units and also needed to manually issue the red cell units. This also meant that staff were unable to enter the units on the EBMS, so their availability was not displayed, and cold chain information was not monitored electronically. The red cell units were finally available for collection at 04:11 the next morning and red cell exchange was commenced at 05:00.
On investigation there was a 4-hour 31-minute delay in blood provision. There were multiple factors that caused this delay which were both clinical and laboratory based. Communication between teams was noted to be good throughout the event. The patient required admission to paediatric ICU, intubation and ventilation with increased oxygen requirement due to the sickle crisis. They recovered and were discharged 14 days after admission.
Learning points
- Unnecessarily assigning specific requirements can cause delays to patient care with life-threatening consequences.
- Risk assessment should be carried out for when information technology (IT) flags are implemented as overridable alerts or hard stops.
- There should be a system in place for identification and triage of urgent samples within pathology departments.
- Appropriate sample volumes should be taken to allow timely laboratory investigation.
ABO-incompatible (ABOi) transfusions n=3
Three laboratory errors resulted in ABOi plasma transfusions, 2 of group O FFP to non-group O patients. One case had an indeterminate group following transfusion of emergency group O red cells, another was a group AB child with lymphoma. The remaining case involved transfusion of group O solvent detergent-FFP (SD-FFP) to a group B neonate.
These cases are discussed in more detail within the supplementary information for Chapter 10, Incorrect Blood Component Transfused (IBCT).
Laboratory errors n=535
As in previous years, most errors occurred at the testing step, 185/535 (34.6%), however in 2025 this was followed by component availability, 125/535 (23.4%) which is the only transfusion step where laboratory errors have not reduced. Component selection, 104/535 (19.4%), was the third most common step (Figure 18.2). Further detail on laboratory errors by step is shown in Table 18.1.
Figure 18.2: Laboratory errors classified by the transfusion step where the primary error
occurred (n=535)
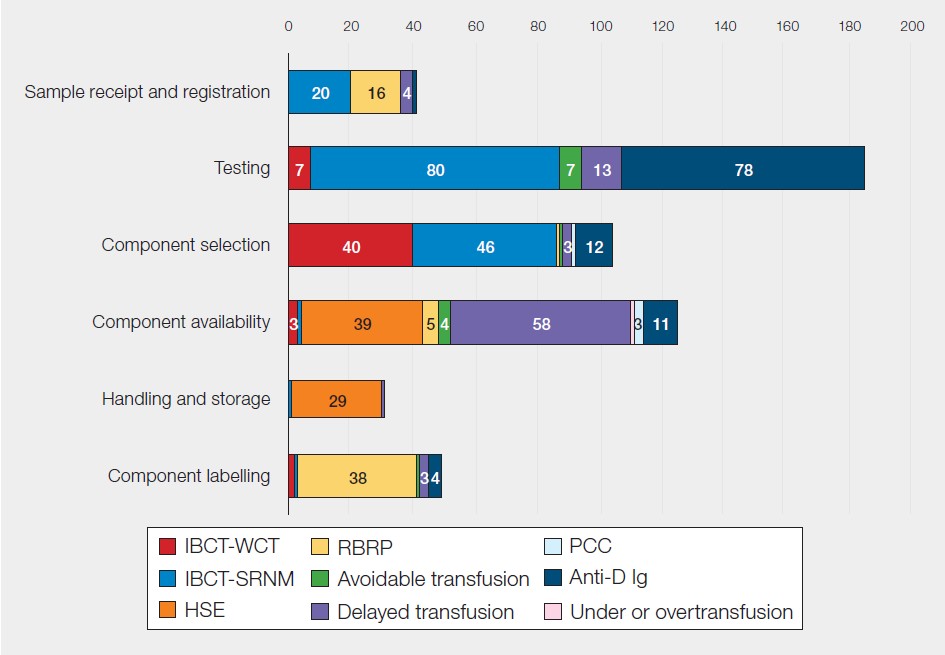
Note: numbers <3 are too small to be annotated on the figure
Errors by step in the laboratory process
Table 18.1: Laboratory errors by step in the transfusion process for 2025 (n=692)
| Transfusion step | Transfused errors | Near miss | Pressure points |
|---|---|---|---|
| Sample receipt and registration n=61 | n=41 | n=20 | – Overlooking information available on request forms or electronic systems – Manual data entry |
| Testing n=196 | n=185 | n=11 | – Lack of knowledge or training resulting in misinterpretation or workarounds – System factors such as lone working |
| Component selection n=153 | n=104 | n=49 | – Not selecting specific antigen-negative components when needed – Lack of provision of D-negative components when required – Gaps in IT to support safe component selection |
| Component labelling n=92 | n=49 | n=43 | – Manual entry of patient details, amending or handwriting – Transposition of labels between components |
| Component availability n=154 | n=125 | n=29 | – Components not available in the expected timeframe causing significant delay with patient impact – Components being inappropriately available to collect after samples or components had expired |
| Component handling and storage n=36 | n=31 | n=5 | – Inappropriately returning components to stock with incomplete cold chain |
Laboratory themes 2025
This year the laboratory learning themes have been matched to the SHOT Transfusion Safety Standards. This aims to show how laboratory practice can align to each standard and their role in improving transfusion safety.
SHOT Safety Standard 1: Transfusion Safety
Specific requirements
IBCT-SRNM is consistently the category in which most laboratory errors occur, and in 2025 accounted
for 149/535 (27.9%) of all SHOT laboratory error reports. These are mostly due to incomplete testing,
44/149 (29.5%), not issuing phenotype or antigen-negative red cells when required, 32/149 (21.5%),
inappropriate use of electronic issue, 23/149 (15.4%) and irradiated components not being provided
when indicated, 22/149 (14.8%). All these situations have the potential to cause significant patient harm such as antibody misidentification, which was implicated in a haemolytic transfusion reaction in 2025.
Incomplete testing was mostly due to incomplete antibody identification, 17/44 (38.6%). The majority of these cases were interpretation errors (10/17), showing that knowledge and process gaps are persisting which impact patient safety. Many of these errors were due to fundamentals of transfusion practice not being applied, with potentially serious patient consequences, as illustrated in Case 18.3.
Case 18.3: Multiple serology interpretation errors lead to lack of blood availability during major haemorrhage
A patient with Hodgkin lymphoma and hemophagocytic lymphohistiocytosis was admitted with a low Hb and was symptomatic. A group and screen (G&S) sample was sent to the laboratory with a request for one adult therapeutic dose of platelets. The antibody investigation was performed overnight with anti-K and anti-e identified. However, the anti-e was misinterpreted as an alloantibody, when it was in fact an autoantibody. The auto control was positive, however this was not noticed. The direct antiglobulin test was also positive but did not trigger any further investigation. Furthermore, anti-e reactivity was not confirmed with two separate examples of positive and negative cells, and no Rh phenotype was performed to confirm specificity in opposition to British Society for Haematology (BSH) guidance, local policies and available decision aids and standard operating procedures (SOP). In the morning, the serology was second checked, but the error was not identified.
On the next day, two units of red cells were requested for the patient. There was only one unit on site that was negative for the combination of alloantibodies erroneously assigned to the patient. Whilst this unit was being crossmatched, the major haemorrhage protocol (MHP) was activated. Alternative red cell units were discussed with the clinical team for possible issue under concession, but the decision was made to wait for blood from the reference centre. The antigen-negative unit was crossmatched and issued to the patient and six further units were urgently transported from the Blood Service, which took 75 minutes.
The patient was treated with volume replacement and was unresponsive. The MHP was stood
down before the patient passed away, and the cause of death was recorded as being related to
the underlying condition. The serology misinterpretation was subsequently highlighted by a third biomedical scientist (BMS) who was performing the outstanding Rh phenotype and identified the patient was e-positive.
The investigation was robust and found many contributory factors such as staff illness, cognitive overload, fatigue, lone working, night working, high workload and time pressures, knowledge gaps and complex serology. The corrective actions were split into immediate, medium- and long-term actions, all of which were system focused. It also highlighted the good practice of the BMS escalating the misinterpretation and good documentation practice.
Learning points
- It is important to consider all aspects of serology when assigning antibody specificity.
- It may be appropriate to consider concessionary release of antigen-positive blood in acute blood loss when fully compatible blood is not available.
- Consider human factors when investigating incidents and planning workload allocation.
Laboratory delays
Delays in the laboratory have reduced to 82/535 (15.3%) from 120/601 (20.0%) in 2024 but remain higher than previous years averages and contributed significantly to the number of errors at the component availability step, 58/125 (46.4%).
Most delays occurred with routine transfusion requests 36/82 (43.9%), followed by urgent 23/82 (28.0%) and emergency 14/82 (17.1%) requests, with the remaining priorities being unknown. This illustrates that practices need to be implemented to improve transfusion care in all circumstances, not just in critical situations. Errors mostly occurred due to communication gaps, 19/82 (23.2%), process deviations, 17/82 (20.7%) or logistical issues, 13/82 (15.9%).
Patient impact of laboratory delays
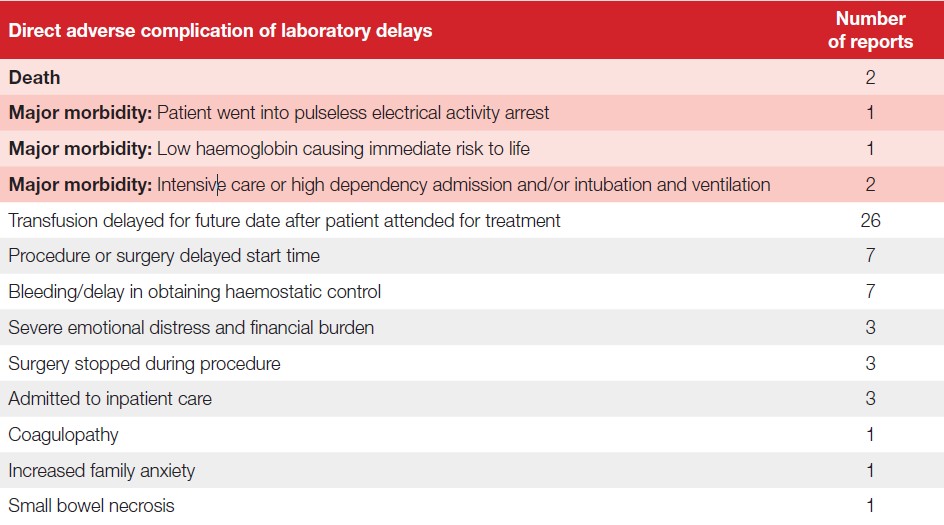
In addition to delays in blood component provision, laboratory errors directly impacted upon patients’ future care or clinical outcome in 58/82 (70.7%) cases (Table 18.2). These cases illustrate the profound, far reaching and often hidden impacts of preventable delays in blood transfusion. Case 18.4 illustrates one such complication and in another case, an organ transplant was delayed due to transfusion of the incorrect group FFP (Case 10.6 in Chapter 10, Incorrect Blood Component Transfused (IBCT)).
Table 18.2: Direct adverse complication of laboratory delays in 2025 (n=58)
Case 18.4: Incomplete communication results in surgery postponement, severe emotional distress and financial burden
An older patient was admitted for total hip replacement in a hospital which was in an isolated
location. A preoperative G&S sample was taken the day before surgery. Due to logistical challenges this did not arrive in the laboratory as scheduled because samples were transported to this site via aeroplane and the flight was cancelled. The surgery was cancelled due to lack of blood availability and rescheduled for a later date. The sample was received by the transfusion laboratory the following evening. There was no communication from the laboratory to the clinical team about the cancelled flight as expected.
The patient had travelled a great distance for the surgery and had arranged for their family member to take time off work and travel to help them postoperatively. The patient was emotionally distressed when they were informed of the rescheduled surgery due to the cost implications to their family member to book further travel. This was the second occasion that the flight had been cancelled, and the laboratory had not communicated with the clinical area. The investigation noted communication challenges between the laboratory and the clinical area.
A further contributory factor noted was that the laboratory did not operate a 24-hour service, and this impacted the timings of replacement flights. There was no defined process within the laboratory regarding contacting the clinical area when transport flights were delayed, but one is now being developed.
Learning points
- There can often be unintended and unforeseen consequences of transfusion delays, which impact patient wellbeing.
- Open and timely communication between healthcare staff improves patient care.
SHOT Safety Standard 2: Transfusion information technology (IT) and
equipment
IT was identified as a contributory factor in 341/535 (63.7%) laboratory errors. This is an increase from 329/601 (54.7%) in 2024. The most common factors were a lack of functionality or algorithms to support safe practice, 77/341 (22.6%), IT could have prevented the error, 45/341 (13.2%) and warning flags in place but not heeded, 38/341 (11.1%). A full breakdown of laboratory IT errors can be found in the supplementary data for this chapter.
SHOT Safety Standard 3: Supporting staff to work safely
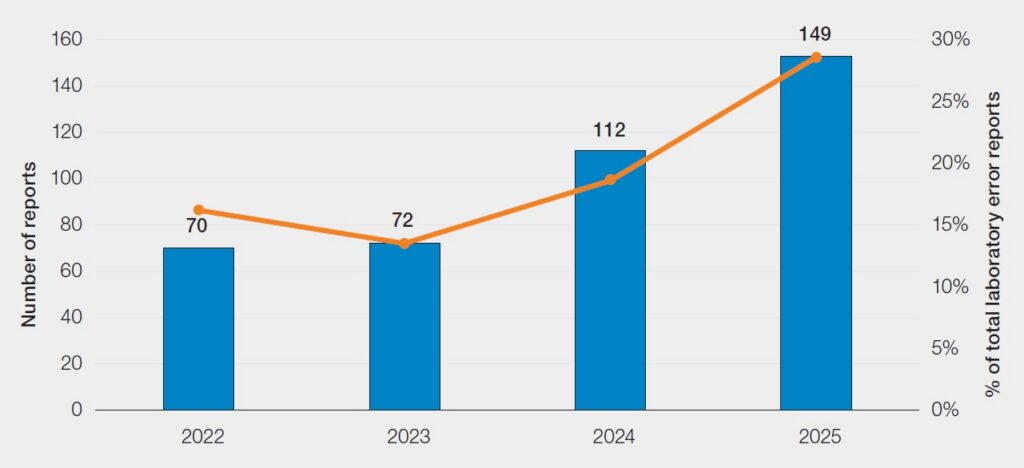
Workload and distribution of workload is a substantial and increasing contributory factor for laboratory errors. A total of 149/535 (27.9%) reports stated that there was a mismatch between workload and staff capacity at the time of the incident; this is an increase from the 112/601 (18.6%) in 2024 and is the fourth consecutive year this has increased (Figure 18.3).
Figure 18.3: Laboratory error reports with staffing and workload mismatch 2022-2025
There may be a disconnect between staffing levels, workload demands, and recorded staffing
requirements. Despite the 27.9% of reports stating staffing and workload mismatch, only 49/535
(9.2%) stated that the capacity plan was not met. It is vital that capacity plans are regularly reviewed and provide a realistic picture of staffing requirements to protect staff and allow safe provision of patient care. An example capacity plan can be found on the United Kingdom Transfusion Laboratory Collaborative (UKTLC) webpage and is available in the recommended resources for this chapter.
The Infected Blood Inquiry (IBI) recommendation 7C states ‘Transfusion laboratories should be staffed (and resourced) adequately to meet the requirements of their functions’ (IBI, 2024). Nearly 2 years on, staffing and workload issues seem to be worsening. Transfusion laboratories are still struggling to obtain proper funding for staffing provision and to recruit and retain staff with an appropriate level of knowledge and experience.
The proportion of reports which stated the member of staff was lone working, covering more than one department or working outside of hours have remained similar to figures reported in 2024 (Table 18.3). These figures represent continued risks, and mitigating actions should be considered to reduce the risks to staff and patients outside of routine working hours (see Case 18.5).
Table 18.3: Contributory factors related to laboratory working patterns 2024 and 2025
| Contributory factor | 2024 | 2025 |
|---|---|---|
| Lone working | 198/601 (32.9%) | 160/535 (29.9%) |
| Outside of routine hours* | 213/513 (41.5%) | 173/429 (40.3%) |
| Covering more than one department | 117/601 (19.5%) | 107/535 (20.0%) |
Case 18.5: Lack of staff support and multiple human factors contribute to component selection error
A female patient was issued a unit of K-positive red cells during a MHP activation in obstetric theatre. Available emergency O D-negative red cells were not used, and standard LIMS processes were not followed, meaning alerts did not appear. The member of staff was lone working outside of routine working hours and the capacity plan was not met at the time. There was also excessive workload due to haematology equipment failures, which had caused a backlog of work.
The member of staff was competency assessed for the procedure, but upon review gaps were found in the SOP. Additionally, the investigation showed that the member of staff had returned from a period of sickness and had not been supported with a return-to-work procedure. Therefore, several personal factors were not highlighted that would have identified them as unfit to return to work at that time. The investigation also discussed a culture where staff felt they were unable to take sick leave when required due to staffing pressures. Many system-focused corrective actions were implemented and included a procedure for return-to-work interviews to be undertaken if the responsible person is not available, additional staff allocation, SOP updates and associated staff training. Workload trends were also reviewed
which resulted in adjustment of late shift time periods to support the busiest working periods.
Learning point
- Supporting staff health, wellbeing and fitness to work also protects patient safety.
SHOT Safety Standard 4: Staff education and training
In 2025 a total of 140/535 (26.2%) reports stated that gaps in skills or knowledge contributed to the
error, which is similar to 2024. This was most evident within HSE and IBCT-SRNM reports (30.9% and
31.5% respectively). However, within all laboratory errors, only 16/535 (3.0%) stated the individual did not have a valid competency assessment for the procedure, with a further 12 reports stating the individual’s competency assessment had lapsed. These figures show that there may be gaps within training material and competency assessments, or that more frequent refreshers or alternative methods of training may be needed. For Health and Care Professions Council (HCPC) registered staff, there is also a level of professional responsibility to speak up and seek guidance when gaps in knowledge could compromise patient care. However, this cannot be the only line of defence, as it is often difficult to identify a gap in knowledge without underpinning awareness.
A lack of appropriate supervision has also been identified as a contributing factor to many laboratory error reports in 2025, 46/535 (8.6%). When combined with skills and knowledge gaps, a lack of supervision creates an environment where staff are unable to raise queries and may make unsafe choices due to this lack of support.
Anti-D Ig errors (n=106)
Almost half of anti-D Ig errors were due to cell-free fetal deoxyribonucleic acid (cffDNA) errors, 51/106
(48.1%). These included 7 false-negatives and 38 false-positives which represent a limitation of technology and cannot be avoided. The remaining 6 cases involved various system issues and are discussed in detail in Chapter 8, Adverse Events Related to Anti-D Immunoglobulin (Ig).
Of the remaining errors, 40/55 (72.7%) were attributed to failure in laboratory processes, 2 cases of result misinterpretation and 2 transcription errors. The remaining 11 cases were due to patients with weak or partial D types. Knowledge gaps underpinned many of these errors, 18/55 (32.7%) and illustrates that anti-D interpretation in pregnancy remains a complex subject and requires focused education initiatives.
SHOT Safety Standard 5: Safety culture
An environment where staff do not feel safe to raise concerns will always adversely impact patient safety. In 2025 only 26/535 (4.9%) reports stated that adverse safety culture contributed to the error. However, as reports are often completed by staff working at management level this may not be a true reflection of transfusion laboratory staff views. In the SHOT/UKTLC culture survey 2023 (SHOT, 2025a), 7.7% staff reported feeling psychologically unsafe in their work environment.
SHOT Safety Standard 6: Patients as safety partners
As laboratory staff are often non-patient facing, it is vital that processes centre the patient and allow staff to feel connected to their positive impact. It is vital that patients are central to their own care decisions and are informed when any care does not meet the expected standard. Within laboratory errors reported in 2025 a total of 20 reports mentioned ‘duty of candour’ being discussed. Thresholds for duty of candour are based on guidance within each country as well as forming part of HCPC standards (HCPC, 2024).
A new SHOT Bite related to duty of candour will be released later in 2026.
SHOT Safety Standards 7 and 8: Haemovigilance and risk management, and
governance
It is encouraging to see that nearly all laboratory errors were investigated and reviewed or were scheduled to be reviewed at a later date, 511/535 (95.5%). Despite this, only 121/535 (22.6%) stated there would be any change to transfusion policy or procedure following the event.
Effective incident investigation and governance require a coordinated, multidisciplinary approach. A
well-established transfusion team comprising of specialist clinical staff, laboratory professionals, and
transfusion practitioners provides the expertise needed to oversee the safe management of transfusion incidents. All transfusion-related incidents should be reported through a single, centralised incident management system to ensure consistency, transparency, and streamlined review. Regular review of reported incidents by the transfusion team enables early identification of trends, system vulnerabilities, and areas requiring improvement.
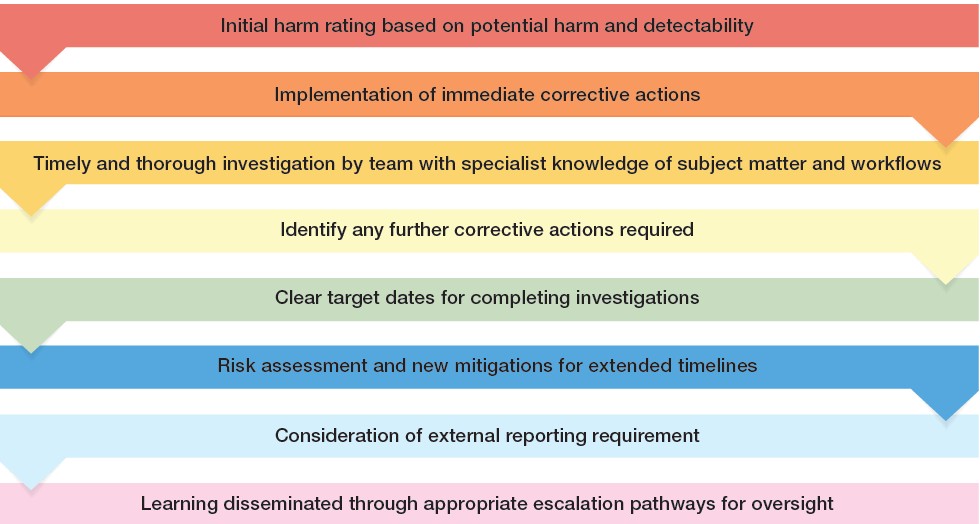
Each incident should undergo an initial risk assessment based on potential harm and detectability,
followed by prompt implementation of any necessary immediate corrective actions. Investigations should be conducted in a timely manner by staff who have a thorough understanding of transfusion systems and workflows. Clear target dates should be set for completing investigations and, where these are not met, risks must be reassessed, and new mitigations and timelines established. The process should also include careful consideration of whether an incident warrants external reporting to bodies such as the Medicines and Healthcare products Regulatory Agency (MHRA) or SHOT. Accurate categorisation of incident types supports effective tracking and trending, while robust escalation pathways through the hospital transfusion committee and wider Trust/Health Board governance groups ensure appropriate oversight and organisational learning.
Examples of effective incident management and governance systems have been provided to SHOT and are contained in the supplementary information for this chapter.
Figure 18.4: Incident investigation flow
Guidance regarding effective governance is intended to be published as part of the actions from the IBI subgroup 7e later in 2026.
Laboratory near misses (NM) n=157
There were 157 laboratory NM reports in 2025 (Figure 18.5). These have decreased from 268 in 2024. Reductions have occurred at every step of the transfusion pathway, with the exception of component
availability, which has increased to 29/157 (18.5%) from 16/268 (6.0%) in 2024.
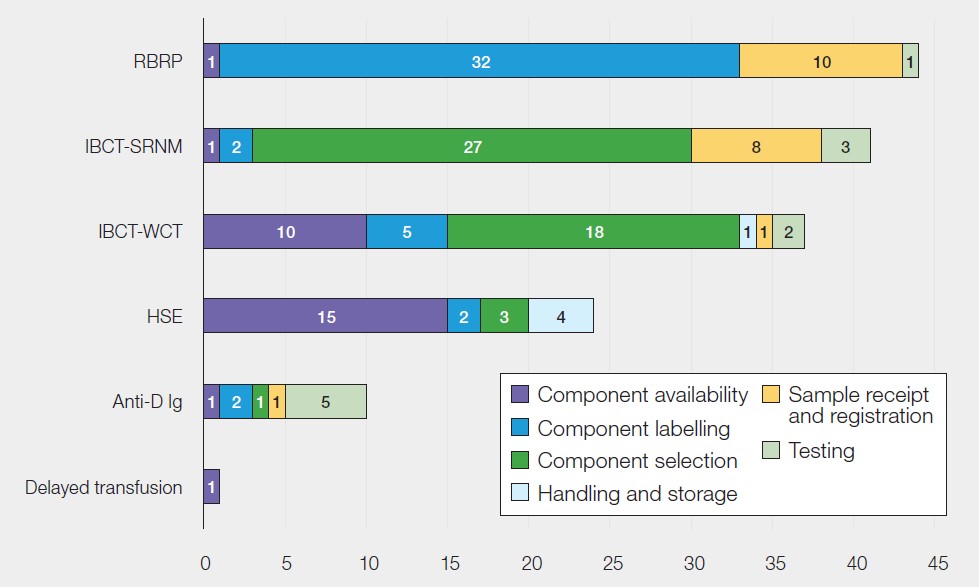
- The largest laboratory NM category continues to be NM RBRP, however these have reduced to
44/157 (28.0%) from 106/268 (39.6%) in 2024. These were 29 labelling errors and 15 patient
identification errors. - NM IBCT-SRNM: 41/157 (26.1%) were the second most common NM laboratory category in 2025:
mostly 22 non-irradiated and 5 not cytomegalovirus (CMV)-negative. - NM IBCT-WCT: 37/157 (23.6%) were 17 wrong group, 17 wrong patient and 3 wrong component
type. - NM HSE: 24/157 (15.3%) included 13 expired units, 4 cold chain errors and 4 reservation periods
exceeded. - NM anti-D Ig: 10/157 (6.4%) included 3 omission or late administration and 3 administrations to the mother of a D-negative infant.
In addition, there was 1 NM delayed transfusion where the member of laboratory staff was uncontactable for over 15 minutes during an acute bleed. The full case description can be found in supplementary material for this chapter.
Figure 18.5: Laboratory NM classified by the transfusion step where the primary error occurred
(n=157)
Conclusion
Whilst overall numbers of laboratory errors have decreased compared to 2024, this has reduced to a
level which is in line with previous years pre-2024. However, harm is far greater than that seen pre-2024, with 2 deaths and 8 cases of major morbidity due to laboratory errors. Patient harm is once again mostly related to delayed transfusions.
Data shows an increase in workload and staffing pressures, which may be influencing the ability to
provide components in a timely manner as well as organisations ability to complete investigation reports. Furthermore, only a very small proportion of laboratory investigations resulted in any changes to policy or procedure, illustrating there may be missed opportunities to implement system improvements and increase patient safety.
The laboratory chapter this year has highlighted the many ways in which insufficient laboratory processes can cause harm to patients and healthcare staff. In some cases, harm has been linked to insufficient staff knowledge and inadequate support systems. The SHOT Transfusion Safety Standards outline criteria for supporting staff to work safely. Without effective mechanisms in place, patients and transfusion staff alike risk being let down by inadequate systems, causing avoidable harm to all involved.
UKTLC update
Author: Kerry Dowling, UKTLC chair
The UKTLC has continued its work with both the IBI recommendations and development of the
Transfusion Transformation Strategy over the last year. The group is currently updating the capacity plan template and accompanying resources as an action from the working group of the 7c recommendation within the IBI report. The next UKTLC survey will be released in 2026, this survey is vital for evidencing the challenges and positive work within transfusion laboratories and we would appreciate participation to enable a full and clear picture.
We continue to update the webpage on the SHOT website with useful resources. We are keen to
continue listening and sharing learning from laboratories and welcome suggestions for resources,
questions and feedback.
UK National External Quality Assurance Scheme (UK NEQAS) update
Author: Megan Jenkins, Katy Veale and Claire Whitham, UK NEQAS Blood Transfusion
Laboratory Practice (BTLP)
Errors made when testing external quality assessment (EQA) samples can feel daunting, but they provide valuable learning opportunities. Because UK NEQAS schemes are educational, mistakes should be seen as ‘free lessons’ that help prevent similar errors when testing clinical samples. The UK NEQAS pre-transfusion testing (PTT) programme continues to highlight issues that are important for improving transfusion safety across the UK.
Procedural errors, especially sample/result transposition, were the most common cause of penalties
in 2025, occurring in eight of ten surveys. Examples included missing an ABO-incompatibility due to
transcription errors and submitting incorrect phenotypes despite selecting the correct interpretation.
Although many laboratories now use automated result transmission, robust processes for manual entry remain essential, particularly during LIMS downtime.
Several laboratories also swapped samples during testing or at the clerical stage, emphasising the need for thorough demographic checks. EQA samples should be handled exactly like clinical samples so that any issues accurately reflect real world risks.
False positive and false negative reactions occurred in nine surveys. Many were linked to procedural
issues such as failing to add plasma or overlooking analyser flags. Laboratories must have clear
procedures for managing analyser warnings and unexpected manual results, as both can compromise patient safety. In some cases, false positives were linked to technology, providing useful evidence for discussions with manufacturers.
Antibody identification errors remain common, particularly in samples containing multiple antibodies. Misidentification was seen in several 2025 exercises, including confusion between anti-D and additional specificities such as anti-Kpa, anti E, anti-Lua, anti-Fya and anti-s. Some uninterpretable (UI) submissions were also rejected due to not meeting guideline criteria. These issues suggest either failure to follow, or misunderstanding of, BSH antibody identification guidance (Milkins, et al., 2013). A systematic approach to inclusion/exclusion is essential. Failure to correctly identify clinically significant antibodies can lead to haemolytic transfusion reactions, highlighting why learning from EQA errors critical.
Recommended resources
SHOT Concessionary Release Toolkit
SHOT Bite No. 37: Recognising the risks of lone working in the laboratory
UKTLC Standards and capacity planning guidance
RCI assist – to aid decision making in reference laboratory referrals (only available in England)
