Authors: Catherine Booth and Claire Wroe
Link to PDF chapter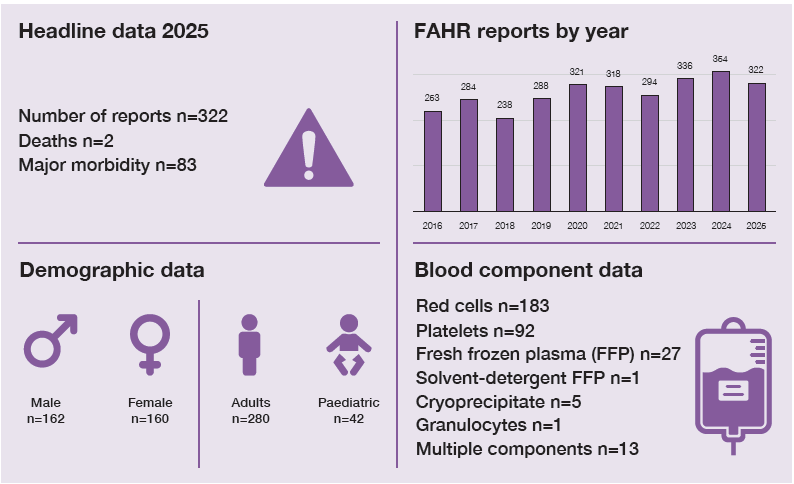
Key SHOT messages
Key findings
- The number of FAHR reports is comparable to previous years.
- There were 2 deaths possibly related to FAHR and 1 patient suffered serious sequelae.
- Inappropriate use of steroids and/or antihistamine to treat febrile reactions continues to occur.
- Repeat serological investigations are often requested when not indicated.
Gaps identified
- Reaction types are not classified based on symptoms, resulting in untargeted treatment.
- A lack of knowledge and understanding of the role of laboratory investigations.
- Knowledge gaps are frequently seen among staff administering transfusions, including those working on haematology wards.
Good practice
- Prompt assessment and management of patients suffering acute transfusion reactions.
Next steps
- Provide feedback to individual clinicians about targeted management of FAHR: sending the SHOT Bites 5a and 5b can help frame this as an opportunity for learning.
- Involve both clinical and laboratory staff in education about FAHR.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
FAHR definition
Allergic/febrile or hypotensive transfusion reactions occurring at any time up to 24 hours following transfusion of a blood component.
For a more detailed definition see https://www.shotuk.org/reporting/incident/definitions/
Introduction
Reactions are classified according to the International Society for Blood Transfusion (ISBT)/ International Haemovigilance Network (IHN) definitions, which are summarised below in Table 20.1, and have been adopted by the British Society for Haematology (BSH) (Soutar, et al., 2023). Mild reactions are not reportable to SHOT.
Table 20.1: Classification of reactions
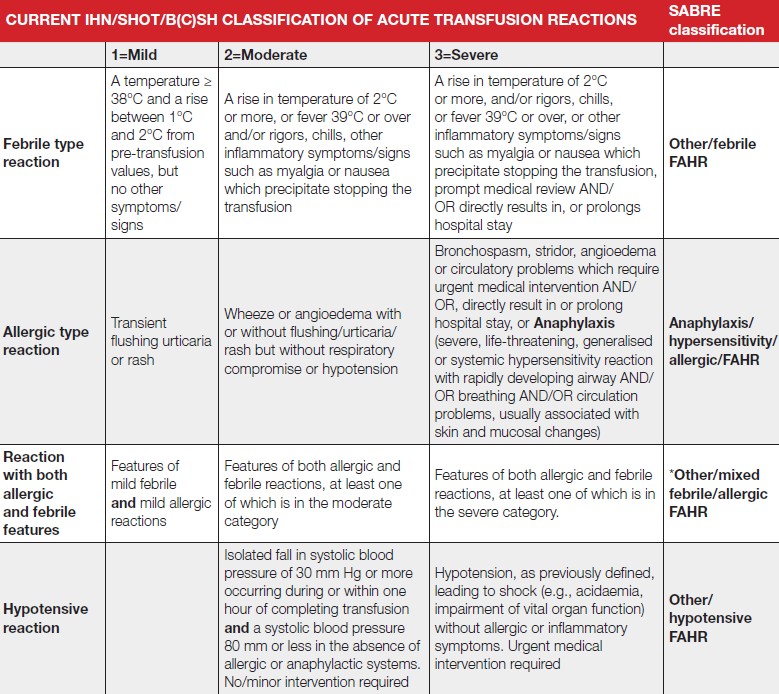
*This category may include mild symptoms/signs of one reaction type providing the other category is either moderate or severe
After an increase in FAHR reports in 2024, the total reported in 2025 has returned to a similar number
to 2020-2023. There were 183 reports related to red cells, 92 to platelets, 27 to fresh frozen plasma
(FFP), 5 to cryoprecipitate, 1 to granulocytes and 14 involving multiple components.
Deaths related to transfusion n=2
There were 2 deaths possibly related to FAHR in 2025. Both involved severe reactions in patients with
other co-morbidities, who had limited physiological reserve.
Case 20.1: Cardiac arrest during transfusion of red cells attributed to possible anaphylaxis (imputability 1 – possible)
A frail elderly patient admitted in a very poor condition had a cardiac arrest during the first 15
minutes of a red cell transfusion. Post-mortem mast-cell tryptase result was markedly elevated, and anaphylaxis due to transfusion (alongside underlying conditions) was considered a likely cause of the deterioration.
Case 20.2: Severe inflammatory reaction in a patient found to have immunoglobulin A (IgA) deficiency precipitates deterioration (imputability 1 – possible)
A patient under investigation for probable lymphoma and with positive blood cultures developed fever, rigors and dyspnoea after 40 minutes of a red cell transfusion. Their blood pressure became unrecordable, requiring admission to intensive care, where they developed progressive multi-organ failure and died 4 days later. Serological incompatibility and bacterial contamination of the unit were excluded. Subsequent investigation showed the patient had severe IgA deficiency with anti-IgA antibodies. It was felt that the acute severe reaction precipitated the deterioration in this already unwell patient.
Major morbidity n=83
The ISBT/IHN classification of a severe reaction has been used to define major morbidity.
Reactions are categorised in Table 20.2.
| Type of reaction | Moderate | Severe | Death | Total |
|---|---|---|---|---|
| Febrile | 147 | 17 | 1 | 165 |
| Allergic | 55 | 59 | 1 | 115 |
| Mixed allergic/febrile | 17 | 6 | 0 | 23 |
| Hypotensive | 18 | 1 | 0 | 19 |
| Total | 237 | 83 | 2 | 322 |
In 14 of the 83 reactions classified as severe, this was primarily because the patient was admitted, or
hospital stay was prolonged.
Although these patients required medical attention, in general there was complete recovery with no
lasting effects. However, 1 patient with underlying cardiac disease suffered severe sequelae when
adrenaline given to treat an anaphylactic reaction to red cells precipitated fast atrial fibrillation and
pulmonary oedema.
SHOT plan to review the criteria for definition of major morbidity in 2026, recognising that many severe acute reactions (particularly febrile type) would not be considered life-threatening.
Following an increase in the proportion of reactions categorised as severe in 2024, the total number and proportion of severe reactions has returned to previous levels. There was a higher number of hypotensive reactions in 2025 compared to previous years, mostly related to red cells (14/19), but only one was severe and this remains a rare reaction type.
Reactions in IgA deficient patients n=7
There were 7 reactions in patients subsequently discovered to have severe IgA deficiency. All were
classified as severe reactions, including one death discussed in Case 20.2. Five of these were febrile/
inflammatory reactions, involving marked systemic upset, 3 of which occurred within the first 15 minutes of transfusion. Two were allergic reactions requiring adrenaline. Four of the patients had experienced reactions previously on multiple occasions. In 3 cases, anti-IgA antibodies were detected, 2 had no anti-IgA antibodies and 2 were not tested.
Anaphylaxis n=40
There were 40 severe allergic reactions requiring treatment with adrenaline. The components most often responsible were platelets (n=16) and FFP (n=16). Children (under 18 years) were disproportionately represented, 13/40 (32.5%). This compares to 42/322 (13.0%) reports related to children in the FAHR category as a whole. One reaction occurred in outpatients, 18 on wards, 3 in the delivery suite and 3 in the emergency department. Severe allergic reactions can occur in unexpected places and without high ratio staffing. In 14 cases, transfusion was being given outside of normal working hours.
Learning point
- All clinical areas giving transfusion must be equipped and staff trained to manage anaphylaxis, and transfusion should only be given overnight when clinically necessary.
Alpha-gal syndrome
Alpha-gal syndrome is an acquired food allergy which develops following tick bites. Immunoglobulin E subtype antibodies formed to alpha-gal can lead to allergic reactions to meat and other animal products (UK Health Security Agency, 2025). These antibodies cross-react with the B blood group antigen, and it has been suggested that this might lead to anaphylactic reactions in non-B/AB patients transfused with group B plasma or platelets (Gilstad, et al., 2023). SHOT is now requesting blood group information for reported allergic reactions to platelets and plasma components as part of international efforts to support or refute a link.
Reaction by component type
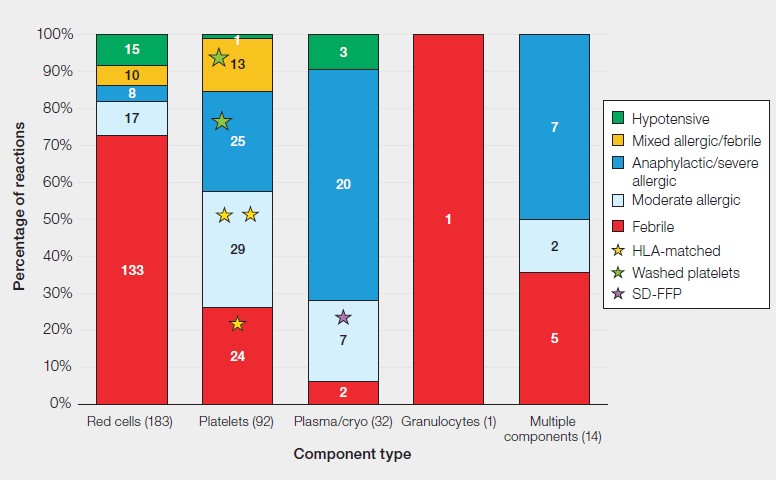
This remains similar to previous Annual SHOT Reports; see Figure 20.1. Red cells are usually associated with febrile-type reactions, 133/183 (72.7%), whereas plasma components and platelets more commonly cause allergic reactions, 27/32 (84.4%) and 54/92 (58.7%) respectively.
Figure 20.1: FAHR reactions by component type in 2025 (n=322)
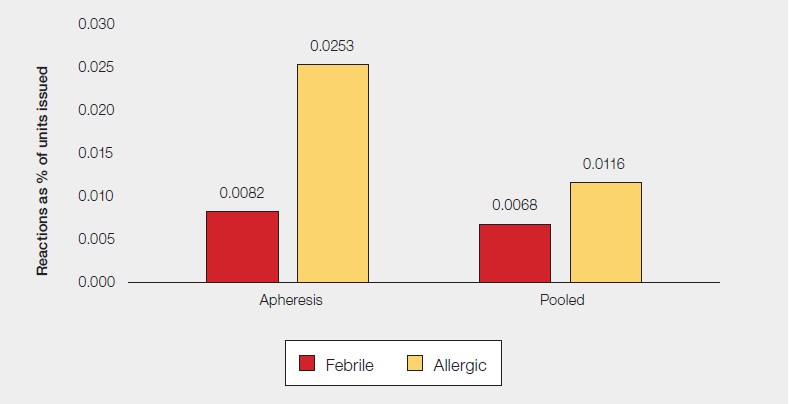
There continues to be a higher incidence of allergic reactions to apheresis platelets compared to pooled platelets (Figure 20.2), related to their higher plasma content (Estcourt, et al., 2017). In 2026, National Health Service Blood and Transplant is commencing a pilot of apheresis platelets suspended in platelet additive solution and plasma, initially in one English region (NHSBT, 2025a). SHOT will be collecting data about this component separately.
Figure 20.2: Incidence of reactions by type of platelet component in 2025
Management of reactions
Of the 165 reactions with only febrile features, 164 provided details of treatment given. Of these, 62/164 (37.8%) were managed inappropriately with an antihistamine and/or steroid where paracetamol alone would have been indicated. This is relatively similar to previous years.
Table 20.3 summarises appropriate treatment targeted to the reaction type, and preventative cover for future transfusion, if needed (Soutar, et al., 2023).
Table 20.3: Targeted treatment for febrile and allergic reactions
| Reaction | Treatment | Prevention of recurrent reactions |
|---|---|---|
| Febrile | Paracetamol | Paracetamol 60 minutes before anticipated time of reaction |
| Allergic | Antihistamine (steroid should not be used routinely) If anaphylaxis, adrenaline is essential | If previous reaction with apheresis platelets try pooled platelets (suspended in platelet additive solution) If reactions continue, give pre-transfusion antihistamine; If reactions continue, consider washed platelets/red cells; For FFP try a pooled component e.g., solvent-detergent treated plasma |
Learning points
- Treatment of febrile and allergic reactions should be targeted to the patient’s symptoms and signs (Soutar, et al., 2023). Febrile reactions can be treated with paracetamol.
- Antihistamines are of no benefit in the absence of allergic features, and even in allergic reactions, steroids should not be used routinely.
Laboratory investigations
There continue to be high rates of untargeted investigations. Repeat group and screen tests were sent
in 271 cases, 71 (26.2%) of these were inappropriate. This included unnecessary serological testing in:
- 41/92 (44.6%) reactions to platelets
- 11/32 (34.4%) reactions to FFP/cryoprecipitate
- 51/115 (44.3%) reactions with only allergic features
Mast cell tryptase was sent unnecessarily in 5 patients with only febrile reactions. In 28 allergic reactions, patient blood cultures were sent, and in 7 cases the unit was cultured.
Case 20.3: Untargeted treatment and investigation of a febrile platelet reaction in a haematology patient
A patient on the haematology ward developed rigors, breathlessness without wheeze and a
temperature rise from 37°C to 38.7°C on completion of a unit of platelets. They were treated with paracetamol, hydrocortisone, chlorphenamine and pethidine. A repeat group and screen and serial mast cell tryptase were sent, along with patient blood cultures. The transfusion incident review team documented a plan for ‘premedication’ before subsequent transfusions.
This febrile platelet reaction would have been appropriately treated with paracetamol alone. Pethidine is not recommended in national guidelines for managing transfusion reactions and it is a strong opiate which carries a risk of respiratory depression. There is no role for red cell serological testing in platelet reactions, and mast cell tryptase is used to support a diagnosis of anaphylaxis where this is unclear clinically. While the precise ‘premedication’ to be used in future was not specified, this often refers to hydrocortisone and chlorphenamine, which would have no benefit for this patient, and there is a risk of cumulative side effects if they receive frequent transfusions.
Learning point
- Red cell serological investigations are only required for febrile or hypotensive reactions to red cells, and where the reaction is severe enough to warrant discontinuing transfusion.
Conclusion
Death or lasting sequelae due to FAHR is rare but does occur. Patients should be warned about the risk of acute transfusion reactions during the consent and shared decision-making process. The potential impact of a severe reaction on a patient who is already clinically vulnerable should be considered when weighing up the decision to transfuse.
It is essential to use the patient’s symptoms and signs to distinguish febrile from allergic reactions. This avoids giving unnecessary medication, which might have side effects, or unnecessary investigations, which could impact on laboratory workflows, lead to delays issuing further blood components, and unnecessarily depleting resources. This should be covered in training for both clinicians and the laboratory and supported by written guidance which is readily accessible and simple to follow.
Recommended resources
Febrile, Allergic and Hypotensive Reactions (FAHR) Cumulative Data page
SHOT Bite No. 05a: Febrile, Allergic and Hypotensive Reactions (FAHR) – getting the
diagnosis right
SHOT Bite No. 05b: Appropriate investigations in Febrile, Allergic and Hypotensive
Reactions (FAHR)
SHOT Video: FAHR – Febrile, Allergic and Hypotensive Reactions
Meet the Experts Webinar: Febrile, Allergic and Hypotensive Transfusion Reactions