Authors: Sharran Grey and Oliver Firth
Link to PDF chapter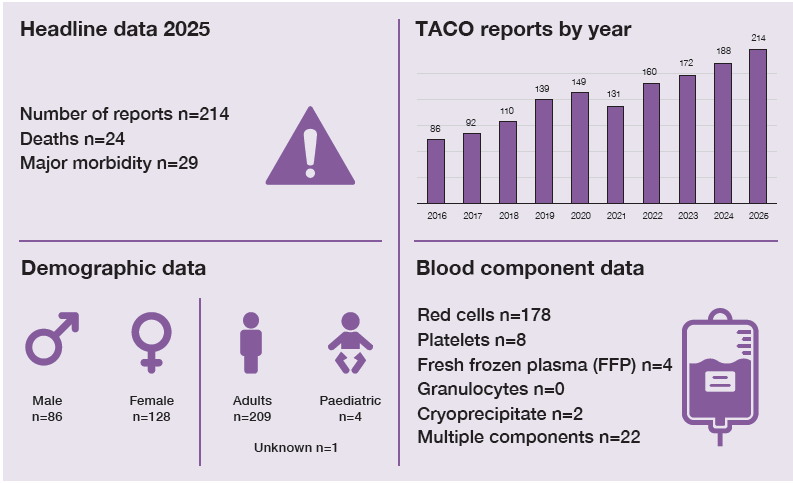
Key SHOT messages
Key findings
- The number of cases reported in 2025 was the highest to date.
- TACO mortality accounted for 11.2% of TACO cases and 44.4% of total deaths.
- TACO caused major morbidity in 13.6% of cases and 18.1% of all reported to SHOT.
- Unnecessary/avoidable transfusion and overtransfusion were factors in ~47% of cases in 2025 (25% in 2024).
- Female patients are disproportionately affected compared to males.
Gaps identified
- The indication for transfusion, informing the appropriate dose of red cells, is not always evident in the cases reported to SHOT and the cause of anaemia is not always identified.
- TACO pre-transfusion risk assessment is not always used, or risk mitigation measures not instituted appropriately despite the identification of risks.
Good practice
- Some evidence of structured local investigation following TACO informing improvements.
- Continued implementation of the TACO pre-transfusion risk assessment into paper and electronic systems.
Next steps
- Organisations should ensure that the correct version of the TACO pre‑transfusion risk assessment is embedded in clinical manuals and electronic systems, supported by educational tools (Figure 21a.2).
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
TACO definition
TACO is defined as acute or worsening respiratory compromise and/or acute or worsening
pulmonary oedema during or up to 12 hours† after transfusion, with additional features including cardiovascular system changes not explained by the patient’s underlying medical condition; evidence of fluid overload and a relevant biomarker¥.
† SHOT accepts cases up to 24 hours
¥ see Table 21a.1 for details of required and additional criteria for the surveillance definition
For a more detailed definition see https://www.shotuk.org/reporting/incident/definitions/
Introduction
The TACO pre-transfusion risk assessment infographic (Figure 21a.1) was updated in the 2024 Annual
SHOT Report (Narayan, et al., 2025) to ensure the appropriate indication and volume of red cell transfusion is a key consideration as a mitigation for TACO. It reflects the updated National Blood Transfusion Committee (NBTC) indication codes which includes code R7 (transfusion for severe chronic anaemia) which emphasises a minimal/single unit transfusion strategy for those patients who are at additional risk of TACO (NBTC, 2024). The TACO pre-transfusion risk assessment is based on real-life haemovigilance data and not traditional research studies. TACO reports are related to a wide range of clinical contexts and patients. These signals offer powerful insights to risk patterns and patient vulnerabilities. Acting on haemovigilance data allows us to adapt our practice, refine risk assessments and implement preventative strategies to improve patient safety. It is a key part of learning from experience and making transfusion practice safer for everyone.
The current version incorporates the changes described above with the aim of improving clarity,
consistency, and effectiveness of application. Specifically, the 2024 and 2025 data provide a clear
signal that inappropriate and excessive volume of transfusion are significant risks in cases of TACO,
which was the main driver for the update in the 2024 Annual SHOT Report. No further change has been made to the TACO pre-transfusion risk assessment in this year’s Annual SHOT Report. Organisations are advised to ensure that the current TACO pre-transfusion risk assessment is in use and staff are trained appropriately about using it effectively.
Figure 21a.1: Current TACO pre-transfusion risk assessment (published in the 2024 Annual SHOT
Report)
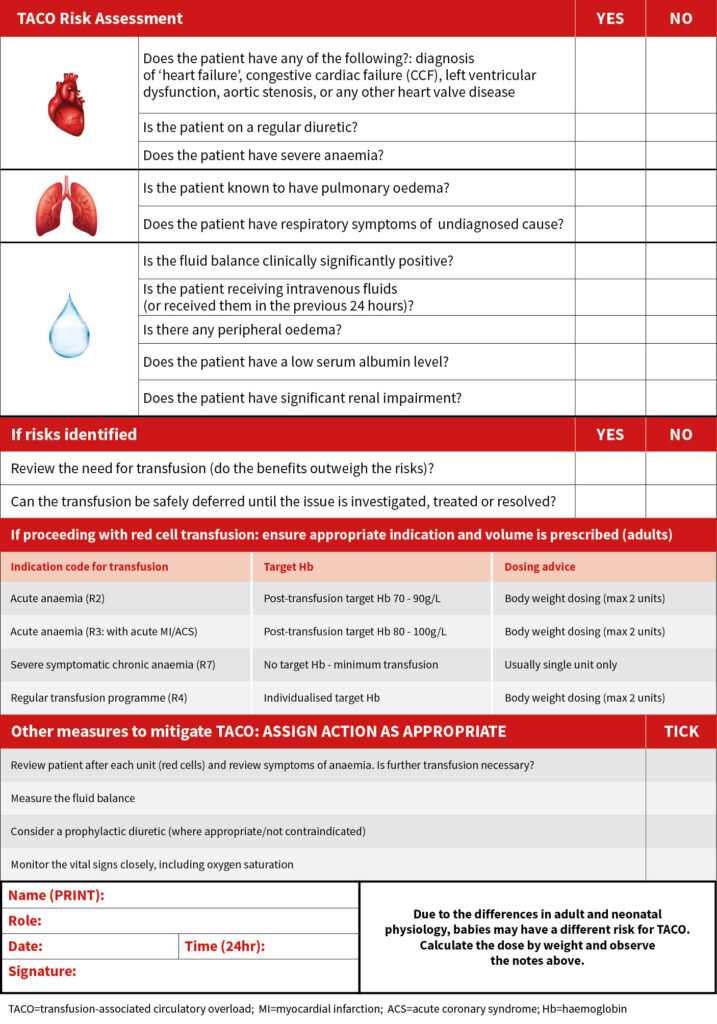
Table 21a.1: TACO surveillance definition (adapted from Wiersum-Osselton, et al., 2019)
| TACO surveillance definition |
|---|
| Patients classified with TACO (surveillance diagnosis) should exhibit at least one required criterion* with onset during or up to 12 hours after transfusion (SHOT continues to accept cases up to 24 hours), and a total of 3 or more criteria i.e., *A and/or B, and total of at least 3 (A to E) |
| *Required criteria (A and/or B) A. Acute or worsening respiratory compromise and/or B. Evidence of acute or worsening pulmonary oedema based on – clinical physical examination, and/or – radiographic chest imaging and/or other non-invasive assessment of cardiac function |
| Additional criteria C. Evidence for cardiovascular system changes not explained by the patient’s underlying medical condition, including development of tachycardia, hypertension, jugular venous distension, enlarged cardiac silhouette and/or peripheral oedema D. Evidence of fluid overload including any of the following: a positive fluid balance; clinical improvement following diuresis E. Supportive result of a relevant biomarker, e.g., an increase of BNP levels or NT-pro BNP to greater than 1.5 times the pre-transfusion value |
The number of cases reported in 2025 (n=214) is the highest to date and is an increase of 26 cases
(13.8%) from 2024 (n=188). Although the pathophysiology of the pulmonary complications of transfusion is not fully understood, the evolving understanding of risk factors for TACO and the development of tools to mitigate risks has advanced significantly in recent years. This chapter describes the demographics of patients reported to have TACO, the adoption of risk-reduction strategies, and highlights areas for further focus based on signals from the data and ongoing trends.
Deaths related to transfusion n=24
TACO‑related deaths decreased in 2025 (n=24; 11.2% of cases) compared with 2024 (n=31; 16.5% of
cases). All 24 deaths in 2025 were imputability 1–2 and accounted for 24/54 (44.4%) of all deaths reported to SHOT.
Peaks in TACO deaths were observed in 2016 and 2020, with the latter possibly related to COVID-19.
There were 15 deaths related to TACO in 2023 which was almost double the number in 2022 (n=8),
and this was a concerning signal in the data that was highlighted in the 2023 Annual SHOT Report
(Narayan, et al., 2024). The trend led to the TACO National Patient Safety Alert (NatPSA) which was
issued in April 2024 (MHRA and SHOT, 2024). This had again doubled in 2024 with 31 deaths where
TACO was implicated (imputability 1 and 2). The cause of this was not clear and was likely multifactorial.
Analysis of the 2024 data showed that 6/31 (19.4%) deaths had evidence of unnecessary/avoidable, or
excessive volume of transfusion, suggesting some cases may have been mitigated or avoided. Although total numbers reduced in 2025, the same analysis showed that 16/24 (66.7%) deaths were potentially avoidable; a higher proportion than in 2024.
The reduction in the numbers of TACO-related deaths is encouraging but it is too early to determine
whether this will continue.
Major morbidity n=29
Major morbidity from TACO decreased in 2025 (n=29; 13.6% of cases) compared with 2024 (n=32;
17.0%). In 2025, these cases accounted for 29/160 (18.1%) of all major morbidity reported to SHOT.
The 2024 figure had represented a marked increase of over 50% compared with 2023 (n=20).
Table 21a.2: Demographic overview of TACO cases in 2025
| Demographic | Number of reports |
|---|---|
| Deaths (imputability 3) | 0 |
| Deaths (imputability 2) | 5 |
| Deaths (imputability 1) | 19 |
| Major morbidity | 29 |
| Age | Range: 2-101 years (4 paediatric patients < 18 years) Median: 76 years |
| Sex | Female=128, male=86 |
| Body weight (adults)* | Female (n=94): mean 63.0kg (range 38.9-116.4kg) Male (n=65): mean 80.6kg (range 40.9-141.0kg) |
| Top 4 medical specialties* | 1st haematology (n=35); 2nd emergency medicine (n=27); 3rd general medicine (n=21); 4th acute medicine (n=16) |
| Intensive care or high dependency units | 18 |
| Day case including community transfusion | 11 |
| Bleeding patients (NBTC indication code R1 or ‘massive bleeding’ indicated) * (NBTC, 2024) | 36 |
| Non-bleeding patients (other NBTC indication codes or ‘not stated’) | 178 |
Female patients continue to be disproportionately affected by TACO: 128/214 (59.8%), and this is likely due to their lower mean body weight compared to male patients. This emphasises the importance of weight-based red cell dosing to avoid over-transfusion. TACO cases occurring in the emergency department has for the first time overtaken general and acute medicine. The reason for this is not clear, however increasing delays in the department contributing to ‘corridor care’ could be a possible factor (RCEM, 2025; RCP, 2025; BMJ, 2026).
Unnecessary transfusion and excessive volume of transfusion: a major contributory factor for TACO and potentially preventable risk
Analysis of 2024 data identified evidence of unnecessary, avoidable, or excessive transfusion volume in 46/188 (24.5%) TACO cases, prompting an update to the TACO risk assessment to include consideration of transfusion indication and volume. In 2025, this proportion increased to 101/214 (47.2%) cases. As transfusion volume, body weight, and pre‑ and post‑transfusion haemoglobin levels are not consistently reported, these figures are likely to underestimate the true scale of the issue. Key contributory factors from the 2025 data are shown here:
- Unnecessary/avoidable transfusions = 43/214 (20.1%)
- Evidence of excessive volume (red cells) = 39/214 (18.2%)
- Evidence of excessive volume (red cells) and possibly unnecessary/avoidable = 19/214 (8.9%)
There has been a large increase in inappropriate and excessive volume of red cell transfusion compared to 2024. This analysis is at odds with the self-reported data on appropriateness of transfusion, where 184/214 (86.0%) were locally assessed as being indicated per British Society for Haematology (BSH) guidelines (Robinson, et al., 2018). Unnecessary and excessive volume of transfusion is a major contributory factor for TACO and potentially preventable risk. The data suggest this is under-recognised in clinical practice, including on retrospective review of cases.
Case 21a.1: Inappropriate/excessive red cell transfusion contributes to a patient’s death (imputability 2 – probable)
A 64kg patient with joint sepsis and pneumonitis was transfused two units of red cells. The indication for transfusion was coded as R3 in accordance with the NBTC indication codes (i.e. acute anaemia in the presence of acute coronary syndrome). The patient’s haemoglobin (Hb) was 80g/L and there was no evidence of acute coronary syndrome. The patient had cardiac comorbidities predisposing to TACO: heart failure, aortic stenosis and regular diuretic use. A TACO pre-transfusion risk assessment was completed, and risks identified, but no specific mitigations were implemented, including questioning the appropriateness or volume of transfusion. The patient developed respiratory compromise with dyspnoea, tachypnoea, and hypoxia (oxygen saturation 81%) requiring 15L of supplemental oxygen. There was tachycardia, hypotension, and a grossly raised N-terminal-pro brain natriuretic peptide
(NT-proBNP). There was no pre-transfusion NT-proBNP level for comparison. The post-transfusion Hb level was 117g/L. The chest X-ray showed pulmonary oedema with possible infection. The patient initially improved following a treatment dose of diuretic but later deteriorated. TACO was cited on the death certificate.
The reporter did not indicate whether this transfusion was locally assessed as inappropriate given R3 was cited as the indication code in the absence of any evidence of acute coronary syndrome (ACS) either by the patient history provided, or on the death certificate. The patient had acute anaemia without evidence of ACS and no active bleeding; therefore, the transfusion trigger should have been <70g/L. The pre-transfusion Hb was 80g/L with no symptoms reported. Even if the pre-transfusion Hb had been 70g/L and the patient was symptomatic, two units of red cells in a 64kg patient would have been an excessive volume to reach post-transfusion target Hb level of 70-90g/L. The post-transfusion Hb in this case was considerably higher at 117g/L.
This case reflects a wider pattern seen in reported TACO cases from 2025 and previous years: inappropriate application of the R3 NBTC red cell indication code. R3 was documented as the indication for transfusion in 28/214 (13.1%) of TACO cases in 2025. On review, clear evidence of an ACS prior to transfusion was present in only 4 cases, with a further 4 providing some supporting evidence. In the remaining 20/28 (71.4%) cases, no evidence of cardiac ischaemia was available, despite use of the R3 indication code to justify transfusion. Within these 20 cases, only 6 could be retrospectively justified using an alternative NBTC indication code. This meant there were 14/28 (50.0%) cases in which transfusion was not indicated under any NBTC category, and 6/28 (21.4%) where transfusion may have been appropriate but the R3 code was incorrectly applied.
The NBTC indication codes are based on current BSH guidelines and are intended to provide a framework to guide evidence-based transfusion practices. In conjunction with appropriate volume of transfusion, this provides an important TACO mitigation strategy. The specifics of the R3 indication code are heavily influenced by the outcomes of the MINT trial (Carson, et al., 2023). This study recruited 3,504 patients and compared restrictive and liberal transfusion strategies in patients with ACS. The trial did not find a statistically significant difference between the two strategies when comparing recurrent myocardial infarction or death at 30 days. It did, however, find statistically higher protocol discontinuation rates in the liberal transfusion group due in part to adverse events including fluid overload and transfusion reactions, along with statistically higher rates of TACO in the liberal transfusion group.
Appropriate use of the NBTC indication codes is clinically important. Patients transfused under R3, in
particular, require meticulous assessment and dosing. The very factor putting them at risk of misclassification – the presence of chronic cardiac disease, 24/28 (85.7%) – is also the comorbidity heightening their vulnerability to TACO. The risk is further compounded by inappropriate selection of R3 over R2 or R7, as use of the R3 indication code is associated with a higher suggested Hb threshold and post-transfusion target, potentially driving larger transfusion volumes in an already high-risk population.
SHOT has attempted to address rising concerns regarding TACO through many different routes, and the TACO incident investigation tool, introduced in 2021, provides a framework for comprehensive review of TACO cases. The aim of the tool is to support identification of gaps that can be addressed locally to improve transfusion safety. Within this tool users must identify whether the transfusion was indicated. The results from 2025 suggest that misunderstanding about the correct use of the R3 indication code is more widespread than prescribers/authorisers of blood transfusion. Only 3/24 (12.5%) reporters identified that the transfusion was either not indicated, or potentially completed under an incorrect indication code.
The NBTC indication codes were originally developed to support audit and quality assurance of transfusion practice. They have since been incorporated into clinical documents, procedures, and IT systems across the National Health Service (NHS) to help guide clinical decision‑making and promote safe, appropriate use of blood components. The codes are aligned with evidence‑based national transfusion guidance, including National Institute for Health and Care Excellence (NICE) and BSH guidelines, and reflect agreed principles of patient blood management.
Review of TACO cases continues to demonstrate potentially avoidable, unnecessary, or excessive transfusion, particularly within the R3 category as highlighted above. While some NHS organisations may not currently mandate use of the NBTC indication codes, the underpinning national guidelines and clinical principles nevertheless apply. Transfusion decisions must always be based on the patient’s overall clinical picture and the underlying cause of anaemia, with careful consideration of risks, benefits, and alternatives, in order to minimise over‑transfusion; especially in patients with acute anaemia and co‑existing cardiac impairment.
Figure 21a.2: Transfusion management of a non-bleeding adult patient – identification of the
cause of anaemia
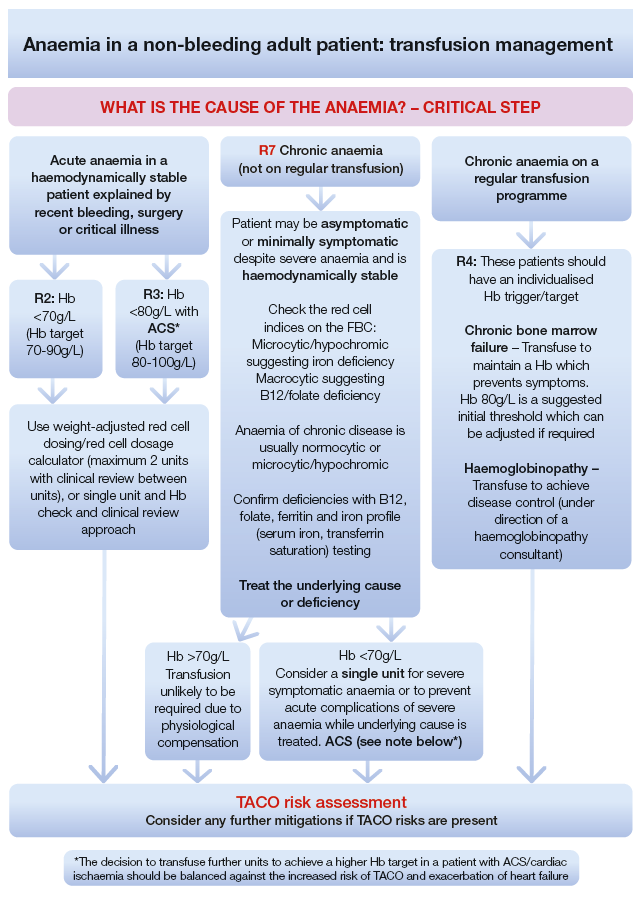
Unnecessary and excessive transfusion are significant contributors to TACO. Determining the correct dose of red cells in a non-bleeding adult patient is a key mitigation for TACO. This is important for all causes of anaemia. The cause of anaemia should be identified to establish the indication for transfusion which then informs the appropriate dose of red cells. A systematic approach should be taken (Figure 21a.2).
Learning points
- Over‑transfusion or unnecessary transfusion should be avoided in patients with acute anaemia. Clinical transfusion practice should be guided by the patient’s overall clinical condition and evidence‑based thresholds. A transfusion trigger (Hb <80g/L) should be reserved for patients with acute cardiac ischaemia (NBTC R3 indication code).
- Severe chronic anaemia (asymptomatic or minimally symptomatic) requires only minimal transfusion (usually a single unit) followed by pharmacological treatment where appropriate. Non-bleeding adult patients with severe chronic anaemia are particularly vulnerable to TACO even in the absence of comorbidities that predispose to TACO.
- In all cases, there should be a systematic approach to the decision to transfuse. The cause
of anaemia should be identified to establish the indication for transfusion, which then informs the appropriate dose of red cells. Risks, benefits and suitable transfusion alternatives must be considered before proceeding with transfusion. These are key factors in mitigating the risk of TACO.
Conclusion
TACO remains a high contributor to major morbidity and mortality, but the current data indicate an
improvement compared with 2024 SHOT data. This is an encouraging sign but it is too early to determine whether it signals a sustainable trend. Unnecessary, avoidable and overtransfusion, particularly of red cells persist along with suboptimal management of severe chronic anaemia. This prompted the TACO NatPSA alert in 2024 (MHRA and SHOT, 2024) which was intended to support organisations in implementing best practice to minimise the risk of TACO.
The pathophysiology and aetiology of pulmonary complications of transfusion is complex and incompletely understood which limits mitigation strategies. However, there are well known risks associated with transfusions which can be mitigated by best practice measures. These include appropriate use of blood, alternatives to transfusion, and correct dose of blood components. The TACO pre-transfusion risk assessment (Figure 21a.1) was updated in the 2024 Annual SHOT Report to promote a systematic approach to red cell transfusion to address modifiable risks for TACO which include avoidable, inappropriate and excessive volume/dose.
It is important to note that TACO can occur with all blood components, not just red cell transfusions.
Therefore, all transfusion decisions should be based on a balanced, evidence‑based assessment of
clinical benefits and risks, with consideration given to appropriate alternatives where feasible.
Organisations are encouraged to adopt the current TACO pre-transfusion risk assessment and associated guidance (Figure 21a.2) in this chapter. Appropriate staff training is essential to ensure accurate use and effective application of the TACO pre‑transfusion risk assessment.
Recommended resources
Transfusion-Associated Circulatory Overload (TACO) Cumulative Data page
TACO pre-transfusion risk assessment (for incorporation into clinical documents)
Transfusion management of a non-bleeding adult patient – identification of the cause of
anaemia
TACO Incident Investigation Guidance Tool
SHOT Bite No. 11: Respiratory symptoms during transfusion
SHOT Video: TACO – Transfusion-Associated Circulatory Overload