Authors: Vera Rosa, Shruthi Narayan and Jennifer Davies
Link to PDF chapter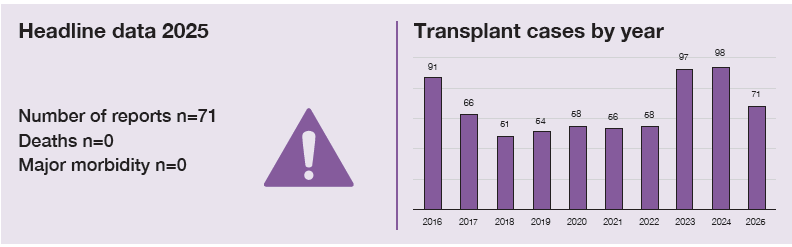
Key SHOT messages
Key findings
- Provision of non-irradiated blood components where required continues to account for the majority of errors in the category incorrect blood component transfused-specific requirements not met (IBCT-SRNM).
- Transfusion of incorrect ABO/D group accounts for most errors in the category IBCT-wrong component transfused (IBCT-WCT).
Gaps identified
- Ineffective, inappropriate or missing flags were identified as contributory factors.
- Lack of interoperability between information technology (IT) systems was noted; reliance on manual entry of transplant protocols and issues with flags contributed to errors.
- Suboptimal shared-care processes, including communication and documentation within the same organisation or between organisations, continue to result in inappropriate transfusions.
Good practice
- Formal investigation with consideration of human factors led to improvements in the system, reducing and preventing a human-centred approach.
- Laboratory processes incorporating a check step of the transplant protocols have been shown to avoid inappropriate transfusion.
Next steps
- Engagement with IT suppliers to assess possible interoperability between different IT systems to reduce the need for manual data entry.
- Report any shared-care improvement that led to a decrease in errors to SHOT acknowledging continuing excellence in transfusion (ACE).
- Electronic patient record (EPR) systems should include care plans and algorithms that support effective communication processes with laboratories, and safe transfusion practice for transplant patients.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
Introduction
The number of haemopoietic stem cell transplants (HSCT) has increased in the United Kingdom (UK) over the past two decades which has introduced new layers of complexity in transfusion especially in cases where the ABO/D group of the recipient and donor differ. Safe transfusions in HSCT and solid organ transplants (SOT) depends on bespoke protocols, effective IT configuration and timely communication across shared-care pathways. Lack of interoperability between IT systems within or across organisations is recognised as a safety risk especially when these require user intervention to enter or act on critical information. In particular, when selection of ABO/D blood components in the laboratory often rely on staff reading notes, flags, or comments without adequate forcing functions. Providing the correct blood component, the correct ABO/D group and meeting the specific requirements are the basics for safe transfusions in this cohort of patients, for whom blood transfusion is an essential life support pre and post transplant.
This chapter solely covers errors related to IBCT errors and near misses (NM) in transplant patients.
Deaths and major morbidity related to transfusion n=0
There were no deaths or major morbidity following transplant-related errors in 2025.
Summary of cases n=71
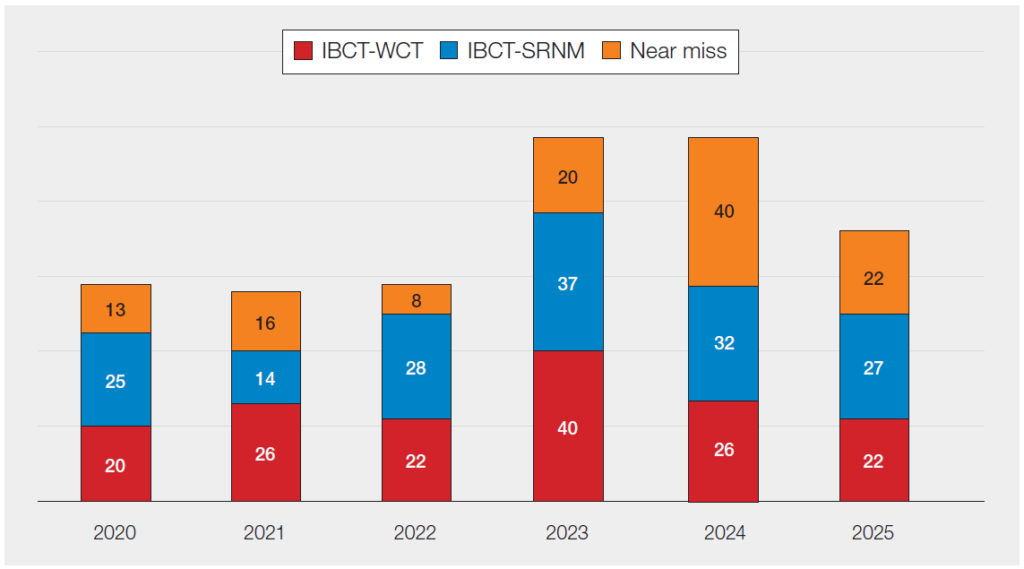
A total of 71 cases are included in this chapter, 22/71 (31.0%) related to IBCT-WCT and 27/71 (38.0%) to IBCT-SRNM. There were 22 NM cases, of these 10/22 (45.5%) related to provision of incorrect blood group, 5/22 (22.7%) related to provision of irradiated components and 2/22 (9.1%) cases of wrong blood in tube (WBIT).
Figure 28.1: Number of transplant-related reports (HSCT and SOT) from 2020 to 2025
Errors involving red cell components represented more than half of the transplant cases where a component was transfused, 32/49 (65.3%). Platelet components accounted for 12/49 (24.5%) reports, plasma components for 2/49 (4.1%) and in 3/49 (6.1%) multiple blood components were administered. The majority of transplant cases were related to HSCT patients, 44/49 (89.8%), with 5/49 (10.2%) being related to SOT involving 2 kidney transplants, 1 liver and 1 lung. The type of organ involved in the transplant was not provided in the remaining case.
IBCT-WCT transplant cases n=22
There were 22 IBCT-WCT cases, of which 18/22 (81.8%) related to laboratory errors and 4/22 (18.2%) from clinical settings. The majority of the laboratory errors occurred during component selection (16/18), mainly leading to a component of the wrong ABO/D group being transfused (15/16). The remaining case related to a patient under 12 months old who received an adult unit for a large volume transfusion which had been irradiated for more than 24 hours. There were 4 component selection errors involving platelets where D-positive units were transfused when D-negative blood components were required. Where errors related to laboratory testing (2/18), in 1 case a dual population in the D-typing was misinterpreted without considering the transplant history (Case 10.7). In the other case, a transcription error led to an ABO-incompatible transfusion where group O fresh frozen plasma (FFP) was transfused to a group A transplant recipient which is described in supplementary information for the IBCT chapter.
The 4 clinical cases were from errors that occurred either at request (2/4), sample taking (1/4) or collection (1/4), 2 related to transfusion of red cells and 2 of platelets. As a result of these events, 2 patients received the incorrect blood group. Two patients received an ABO-compatible blood component of which one involved transfusion of a blood component intended for a different patient and the other case blood was intended for the patient transfused but issued on a sample which was later found to be a WBIT.
Human factors and IT impact in IBCT-WCT
In 7/22 cases there was a delay in adding the transplant protocol information or appropriate flag to the laboratory information management system (LIMS) which led to an incorrect blood group being selected and transfused. This highlights the risks associated with processes that rely on manual entry of information into electronic systems. Lack of interoperability between EPR and LIMS was also identified.
Visual flags that were not actionable and could be easily overridden were identified in 5/22 IBCT-WCT cases. This reflects the inefficiency of flags when the algorithm does not enforce alerts or flags to be hard stops or require an action from the user. One case in which D-positive platelets were issued when D-negative blood components were required related to failure to discuss the urgency of the transfusion with the haematology consultant for concessionary release. One of the contributory factors in this case related to the national blood shortage in England. This resulted in laboratory staff prioritising avoidance of component wastage and selecting alternative blood components without seeking clinical input.
Case 28.1: Incorrect manual entry of donor blood group leads to D-sensitisation
A male patient with blood group A D-positive received an allogeneic A D-negative HSCT. The transplant protocol was inputted onto the LIMS 7 days post-transplant, but the blood group of the donor was incorrectly entered as A D-positive with no reconciliation between the donor and recipient records. The patient was transfused with several A D-positive blood components. Over four years later, a group and screen sample was taken which revealed that the patient’s blood group had changed to the donor’s group of A D-negative and immune anti-D developed.
Case 28.1 shows the potential impact of manual data entry errors of information that triggers algorithms for correct blood selection. In this case, the patient received incorrect D-positive blood components leading to sensitisation to the D antigen.
A case of a cancelled renal transplant following an increase of ABO antibodies due to inappropriate transfusion is described in Chapter 10, Incorrect Blood Component Transfused, Case 10.6.
Learning points
- The presence of immune anti-D can lead to potential delays in provision of blood components.
- Lack of interoperability between IT systems requiring manual entry by the users can potentially contribute to suboptimal care.
IBCT-SRNM transplant cases n=27
There were 27 IBCT-SRNM cases, 19/27 (70.4%) clinical and 8/27 (29.6%) laboratory events. All the clinical errors occurred during request whereas the laboratory errors were during sample receipt and registration (3/8) and testing (5/8). Failure to provide irradiated blood components was the most common error accounting for 16/27 (59.3%) cases. Other errors reported were inappropriate use of electronic issue of red cells (4/27), provision of blood components when testing had not been completed (3/27), failure to provide human leucocyte antigen (HLA)-matched platelets (3/27) or antigen-negative red cells (1/27).
Human factors and IT impact in IBCT-SRNM
In 18/27 IBCT-SRNM cases, ineffective shared-care processes within or between different organisations was the greatest contributory factor to the event. Where errors occurred within the same organisation, they were mostly due to the clinical team not informing the laboratory of the specific requirements or not sending this information in a timely manner. There were 2 cases where assumptions were made that another department or healthcare professional had already informed the laboratory. Gaps in communication and inaccurate documentation were noted in shared-care cases involving different organisations. Lack of interoperability between IT systems was identified in 3 cases and the incorrect use or unavailability of appropriate flags were mentioned in 8. Flags being easily overridden or not added correctly were common themes. In 3 cases, LIMS downtime due to a cyber-attack impacted the laboratory workflow and increased pressure to provide blood components in a timely manner. This also impacted the alerts available in the clinical IT system used at pre-administration.
Case 28.2: A patient highlights the need for a specific requirement in platelet transfusion
A HSCT patient emphasised to their clinical team that they needed HLA-selected platelets. This information was not acted upon and the patient received an adult therapeutic unit of platelets that did not meet this specific requirement. Following investigation, it was identified that none of the shared-care documentation sent by the referring hospital mentioned this requirement. The Blood Services were contacted and confirmed that HLA-selected platelets had been previously provided to the original treating hospital.
Case 28.2 shows the importance of listening to patients and confirming the information communicated by them. In this case, the patient spoke up about their requirements for blood transfusion, but it was not acted upon before the transfusion commenced.
Learning points
- Healthcare professionals should advocate for active patient participation in their own care.
- Shared-care processes between different organisations and within departments must ensure that all relevant information is complete, accurate, clear and provided in a timely manner.
Near miss summary n=22
There were 22 NM cases related to transplant patients; 17 laboratory and 5 clinical events, including 2 WBIT. NM IBCT-WCT (14/22) cases could have led to transfusion of the wrong ABO/D group (10/14) or an incorrect patient being transfused (4/14). One of the cases would have resulted in an ABO-incompatible transfusion if the error had not been detected before transfusion. Failure to provide irradiated blood components accounted for 5/6 NM IBCT-SRNM reports with the remaining case related to failure to provide washed platelets.
Conclusion
The transfusion requirements for HSCT and SOT patients are complex especially in ABO/D mismatched transplants. For effective and optimal care all relevant information must be shared across all departments involved in the patient’s care, either within teams in the same organisation or with external organisations such as the transplant centres. Shared-care pathways must ensure that communication is clear, accurate and occurs in a timely manner.
IT systems and suppliers can help prevent these errors by bridging the gaps in interoperability and supporting algorithms that promote safe practice. Manual entry of flags and transplant protocols is a recognised safety risk associated with potential transcription errors and misinterpretation of information. EPR systems should support safe practice for communication of information to laboratories, along with ordering and prescription/authorisation of correct components. But foremost, organisations and departments must ensure that staff have the appropriate knowledge related to the transfusion requirements for these patients. Adequate staffing levels and opportunities for learning, embedded within safe systems to provide best care, are paramount for transfusion safety.
Recommended resources
SHOT Video: Tools supporting safe and effective communication
SHOT Bite No.18: Transfusion errors in haemopoietic stem cell transplant patients (HSCT)