Authors: Shruthi Narayan with input from members of the SHOT team
Link to PDF chapterGlossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
Key SHOT messages
- Meeting the SHOT Transfusion Safety Standards and addressing gaps identified in the Infected Blood Inquiry (IBI) report recommendations: Delivering safer transfusion care now requires urgent, coordinated action to embed the SHOT Transfusion Safety Standards, close longstanding system and practice gaps highlighted by the IBI, and ensure organisations receive the resources and prioritisation needed to protect both patients and staff.
- Safe, informed transfusion decisions: Transfusions are safest when used appropriately. All staff must understand indications, alternatives, risks, benefits and potential reactions relevant to their role. Unnecessary transfusions should be avoided, and patients (and carers) must be clearly informed and involved in decision-making.
- Addressing transfusion errors: Errors continue to account for the majority of SHOT reports. Communication issues, assumptions, distractions, staffing pressures, suboptimal information technology (IT) and weak safety culture continue to drive avoidable harm. Learning from safety events should be optimised, guided by human factors principles, with meaningful system-level improvements implemented.
- Resourcing clinical and laboratory teams: Safe transfusion requires adequate, trained staff and resilient systems. Services must plan for peaks in workload whilst maintaining minimum safe staffing to protect quality of care, avoiding staff fatigue and burnout.
- Closing knowledge gaps and reducing cognitive bias: Staff training must go beyond technical transfusion knowledge. Staff need to be aware of the fundamentals of patient safety, human factors, and quality improvement, with explicit understanding of how cognitive bias shapes decision-making and how to mitigate it.
- Clear, usable policies and processes: Guidelines, standard operating procedures (SOP) and decision aids must be simple, up to date, accessible, easy to follow and explain the rationale behind each step. When processes are intuitive and aligned with national guidance, staff are more likely to engage and less likely to create workarounds.
- Strengthening safety culture: A just, restorative, learning culture is essential. Staff must feel able to raise concerns, report incidents and suggest improvements without fear of reprisal. Regular measurement of safety culture and its impact on patient and staff wellbeing, is key to driving timely action. Open and transparent partnership with patients is vital to ensure meaningful changes to the way care is delivered.
- Ensuring safe shared care: Clear, complete, and timely communication across teams and organisations is critical. Safe transfusion depends on robust information transfer across the entire patient pathway.
- Performing essential safety checks: The pre‑administration check at the patient’s side is the final, crucial safety barrier: confirming the right patient receives the right component with the right specification. The transfusion-associated circulatory overload (TACO) pre-transfusion risk assessment enables early mitigation for vulnerable patients. These checks are protective pauses, not tick‑box tasks.
Recommendation
- All healthcare organisations should proactively identify gaps in transfusion safety by benchmarking their practices against the SHOT Transfusion Safety Standards, implement targeted improvements, and continuously monitor compliance through structured audits and performance indicators to enhance safety for both patients and staff.
Introduction
As SHOT marks its 30th year of continuous haemovigilance, this milestone offers a moment to
reflect on what three decades of collective effort have achieved, and what the data now demand
from everyone in healthcare. Over the years of SHOT reporting, several reassuring signals stand out:
transfusion‑transmitted infections remain exceptionally rare; ABO‑incompatible transfusions continue to decline; and once-devastating reactions such as transfusion-associated graft-versus-host disease (TA‑GvHD), post-transfusion purpura (PTP), and immune‑mediated transfusion-related acute lung injury (TRALI) have markedly reduced following sustained system improvements. These gains did not occur by chance, but through the commitment of thousands of staff to report incidents, challenge unsafe systems and embed learning into everyday practice, building a national transfusion safety culture capable of detecting risk where care is delivered.
Yet the 2025 data continue to show that the healthcare system remains under growing pressure. Errors still dominate the landscape, 83% of all SHOT reports, including persistent wrong blood in tube (WBIT) events, and preventable harm from delayed, under and overtransfusion continues to rise. Pulmonary complications, febrile and allergic reactions remain prevalent, and one definite fatal haemolytic reaction occurred this year despite the overall rarity of fatal events. These trends mirror recurrent systemic vulnerabilities: workforce shortages, inconsistent training, ageing IT infrastructure and variable safety culture. Despite longstanding national initiatives, transfusion practice in the National Health Service (NHS) continues to expose patients to avoidable risk, underscoring the urgent need for digital transformation, workforce investment and strengthened oversight (Murphy & Toh, 2026).
SHOT’s Transfusion Safety Standards, launched in July 2025, offer a clear, measurable framework to
strengthen safety, governance, staffing, digital capability and patient partnership. But progress is variable and constrained by the lack of dedicated implementation funding. The message at 30 years is clear: a back‑to‑basics focus on patient identification, documentation and teamwork must be matched with real investment in modern systems, protected learning time and strong leadership. Haemovigilance remains the NHS’s pulse check; able to sense when the system is faltering. Acting on that signal is now essential to enable the next three decades of safe transfusion practice.
The IBI exposed significant and systemic failings in transfusion safety that spanned for decades, particularly in the 1970s-1990s, leading to thousands of avoidable infections with human immunodeficiency virus and hepatitis C (IBI, 2024). The contaminated blood crisis stands as a stark reminder of the critical importance of safe transfusion practice. As the Inquiry’s wide‑ranging recommendations are now being implemented, we have a responsibility to ensure that the lessons learned are not lost. This is a pivotal moment to embed those recommendations, strengthen transfusion safety, and build systems that prevent such a tragedy from ever happening again.
Safety is not merely a policy requirement. It is a shared professional commitment that protects both
patients and staff.
SHOT Transfusion Safety Standards
The 2025 SHOT Transfusion Safety Standards are a major milestone in the United Kingdom’s (UK)
approach to transfusion safety. This represents a shift from reactive learning based on annual incident reports to a proactive, structured framework that aims to embed safety and quality throughout the transfusion process (see ‘Recommended resources’). SHOT haemovigilance data has repeatedly demonstrated that transfusion‑related harm is predominantly caused by preventable errors rather than the intrinsic risks of blood components. Errors such as patient misidentification, sample mislabelling, communication issues, and insufficient patient monitoring continue to occur despite the existence of guidance. Variability between organisations, fragmented governance, and inconsistent translation of learning into practice further reinforce the need for formal standards. Additionally, national patient‑safety reforms and the findings of the IBI highlighted gaps in governance, accountability, and patient involvement; key drivers behind the creation of these standards.
The development of the standards drew on repeated themes from SHOT reports and incorporated wide stakeholder engagement, including clinical teams, laboratory staff, transfusion practitioners, regulators, and patient representatives. They were also deliberately aligned with existing national and international guidance to avoid duplication and instead consolidate all relevant safety expectations into a coherent framework. The standards are organised across key domains: governance and leadership; education and competence; safe systems; incident reporting and learning; patient‑centred care; and culture and continuous improvement, providing a comprehensive template for what reliable, safe transfusion practice should look like. Each domain outlines essential requirements. These include strong organisational accountability; consistent training and competency assessment; digital and procedural safeguards such as positive patient identification and electronic systems; psychologically safe reporting cultures; clear, inclusive patient information and involvement in decisions; and continuous improvement driven by data and shared learning. Together, these are intended to support organisations in both assessing their current performance and driving targeted improvement.
Figure 4.1: The core domains of the SHOT Transfusion Safety Standards

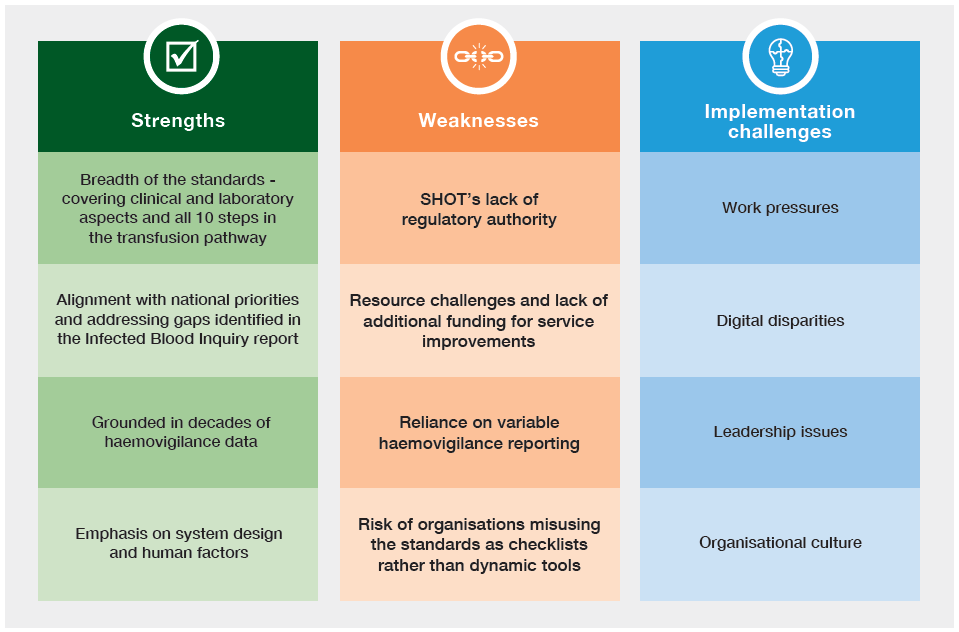
Qualitatively, the standards offer a shared language, strengthen cross‑disciplinary understanding, and emphasise systems thinking and staff wellbeing. Quantitatively, they can be mapped to indicators such as WBIT events, turnaround times, training compliance, psychological‑safety measures, and patient‑experience metrics, providing a basis for measuring progress. Figure 4.2 covers some of the key strengths, weaknesses and implementation challenges relating to the SHOT Transfusion Safety Standards.
Figure 4.2: SHOT Transfusion Safety Standards: key strengths, weaknesses and
implementation challenges
Here are some key next steps for embedding the standards: conducting local gap analyses; aligning
governance and reporting structures; ensuring sufficient staffing, training time, and digital capability;
involving patients in co‑design; and evaluating and sharing learning over time. The SHOT Transfusion Safety Standards condense three decades of learning into a practical, forward‑looking framework and calls on leaders, clinicians, scientists, and patients to use them to drive the next generation of safe transfusion practice.
Updates from the 4 UK nations regarding implementation of the SHOT Transfusion Safety Standards:
England (update provided by Dr Shubha Allard)
The SHOT Transfusion Safety Standards promote consistent best practice informed by decades of UK
haemovigilance data and are designed to address recurrent causes of transfusion error by strengthening governance, embedding evidence‑based practice, and promoting a consistent safety culture. They emphasise proactive risk management, robust accountability, and the importance of adequately trained staff throughout the transfusion pathway. In doing so, they directly address known system vulnerabilities, including procedural non‑compliance and IT failures, and translate national learning into sustained improvements in practice. The themes align with key priorities within the current Transfusion Transformation strategy being drafted for England. The SHOT Transfusion Safety Standards will also be central to a scoping initiative currently underway for the development of a Transfusion Safety Framework for Pathology Networks. NHS organisations are at varying stages of completing gap analyses that will guide the prioritisation of improvement efforts.
Scotland (update provided by April Molloy)
Scotland is currently strengthening blood transfusion safety by implementing the recommendations of the SHOT Transfusion Safety Standards and the IBI. In August 2025, the Scottish Government’s Director of Population outlined clear expectations for leadership and governance in a letter to Health Boards (Boards). This letter stated that each Board must appoint an Executive Director with overall responsibility for implementation and empower hospital transfusion committees (HTC) with the authority and support needed to implement required changes. National issues will be escalated through the Scottish National Blood Transfusion Committee. To support the implementation of the standards, existing governance processes were to be used initially. Boards were directed to submit a completed SHOT baseline assessment of the standards by 20 February 2026 and to begin improvement planning based on the findings. Following submission, compliance will be monitored through a period of national ‘light touch assurance’ before transitioning oversight to routine Board governance arrangements if the Scottish Government feels suitable arrangements are in place.
Wales (update provided by Rachel Borrell and Stephanie Ditcham on behalf of the Blood Health National Oversight Group (BHNOG))
Following the publication of the SHOT Transfusion Safety Standards in July 2025, and in alignment
with Recommendation 7e of the IBI, a Welsh Health Circular was published on 2 October 2025 by the
Deputy Chief Medical Officer for Wales and the Chair of BHNOG (Welsh Government, 2025). The circular aimed to strengthen governance requirements and board‑level oversight by directing Health Boards to embed these standards within their patient quality and safety governance structures, and to work with their HTC to complete the baseline gap analysis and implement the actions needed to address any non‑compliance and drive continuous improvement. The national Transfusion Risk Group, which includes representatives from all Welsh Health Boards, acts as the governance reporting route to BHNOG, with escalation to NHS Performance and Improvement as required. Common areas of non‑compliance have been identified across Wales, and collective national actions are to be developed to address these issues.
Northern Ireland (update provided by Dr Allameddine Allameddine, Northern Ireland Blood Transfusion Service (NIBTS) and Dr David Millar, Northern Ireland Transfusion Committee (NITC))
NIBTS has discussed the SHOT Transfusion Safety Standards with the regional IBI Working Group,
chaired by the Department of Health, and the standards have been agreed in principle, consistent with the approach taken across the other devolved nations. The proposals have also been shared with NITC colleagues, and following the NITC meeting on 12 November 2025, the standards were formally endorsed on behalf of Northern Ireland. Regional gap analyses for the SHOT Transfusion Safety Standards have commenced, recognising the cross‑trust nature of transfusion safety in Northern Ireland, particularly in the context of Right Patient, Right Blood, Encompass, WinPath and future BPaT implementation. All of these are regional transformation programmes used across NI Trusts and Trusts have been asked to review the regional gap analyses via their HTC and provide feedback. Together, these programmes underpin regional approaches to Right Patient, Right Blood and interoperability, and they should be become highly relevant to the implementation of the SHOT Transfusion Safety Standards in Northern Ireland. Engagement with Regulation and Quality Improvement Authority has begun, and it is planned to bring the standards to the Northern Ireland Blood Oversight Group to support coordinated implementation, alignment and compliance across the region.
Effective leadership and governance for transfusion practice
Effective, compassionate, and shared leadership, underpinned by robust and integrated governance,
is essential to ensuring safe and reliable transfusion practice across the UK. The findings of the IBI
exposed critical and longstanding gaps in governance, including fragmented accountability, lack of
transparency, delayed responses to emerging risks, and insufficient incorporation of patient voice,
all of which contributed to avoidable harm (IBI, 2024). These findings highlight the urgent need to
strengthen transfusion governance frameworks so that they are proactive, coherent, and responsive
across organisational and national boundaries. Contemporary evidence suggests that these challenges persist: the National Blood Transfusion Committee survey of Hospital Transfusion Committees (NBTC, 2025b) demonstrates ongoing variability in committee effectiveness, engagement, and influence, reflecting wider inconsistencies in governance maturity and prioritisation of transfusion safety across the UK. Such variation, compounded by workforce pressures and system complexity, underscores the importance of leadership approaches that foster psychological safety, multidisciplinary collaboration, and openness, while actively mitigating risks such as groupthink in clinical decision-making (West, et al., 2014). Importantly, there is an inextricable link between staff wellbeing and patient or donor safety, necessitating governance systems that prioritise not only safe processes but also the conditions in which staff can work safely and sustainably.
In this context, the focus of the IBI recommendation 7e subgroup is to address these identified gaps
and strengthen transfusion governance across the UK. However, it is important to recognise that merely refreshing terms of reference or producing a framework will not, in isolation, deliver meaningful or sustained change in how transfusion is led, managed, and governed. Achieving tangible improvement requires collective action, bringing together the entire transfusion community alongside patient safety, risk management, quality, and governance teams. Together, it is imperative to co-create and embed systems of compassionate governance that actively listen, respond, and adapt. Only through such coordinated, inclusive, and action-oriented efforts can we ensure enhanced safety for donors, patients, and staff, and realise the ambition of a truly learning healthcare system.
Update on the progress with implementation of 7e
recommendation from the IBI Report
With the SHOT Transfusion Safety Standards now released, efforts are shifting towards strengthening
and improving the governance mechanisms that will support their implementation across the UK. SHOT continues to work closely with stakeholders to identify practical, sustainable solutions to long‑standing safety concerns, including workforce pressures, laboratory systems, and transfusion IT. This collaborative approach aims to foster a culture of continuous improvement and shared responsibility across all organisations involved in transfusion.
A key recommendation within Section 7 of the Inquiry’s Patient Safety chapter relates directly to the
implementation of SHOT recommendations. It states:
(7e) That all NHS organisations across the UK have a mechanism in place for implementing recommendations of SHOT reports, which should be professionally mandated, and for monitoring
such implementation.
This recommendation underpins the current focus on strengthening governance, ensuring that
organisations not only adopt SHOT Transfusion Safety Standards but can also demonstrate and monitor their implementation and compliance in a consistent and accountable way.
The 7e subgroup is focused on strengthening transfusion safety and governance across the NHS through three major deliverables which are aimed to be completed by the end of 2026:
- An effective governance framework for transfusion in hospitals fully integrated into patient
safety governance - A Transfusion Safety Framework for Pathology Networks to standardise and support safe
systems at network level - A HTC Operational Toolkit to improve consistency, functioning, leadership and structure of HTC
activities
These deliverables aim to reduce unwarranted variation, optimise transfusion practice, and support
shared leadership and UK‑wide collaboration. Despite progress, significant challenges remain, particularly the absence of funding and the future need for coordinated implementation support across the NHS.
The 7e subgroup continues to emphasise:
- Shared leadership across professional groups, organisations and systems
- UK-wide representation, ensuring solutions are applicable and equitable
- Collaboration and communication, acknowledging the wide stakeholder landscape (Care Quality
Commission and equivalent across the UK, the Medicines and Healthcare products Regulatory
Agency (MHRA), NHS England, SHOT, Pathology Networks, Integrated Care Boards, clinical teams) - Recognition that real challenges lie ahead, particularly around implementation without new funding streams
The biggest question remains:
Once the governance framework is released in late 2026, how do we ensure it is implemented
consistently and effectively across every NHS hospital and network?
The 7e subgroup has made strong progress despite funding constraints. All the key deliverables form
the foundation for safer, more consistent transfusion practice across the NHS. Collaboration across
organisations, professions and nations remains pivotal, and successful implementation will require clear accountability, strong communications and coordinated leadership once the framework is released.
Improving patient consent and shared decision-making
Despite increased national focus, consent and shared decision-making in transfusion practice remain
suboptimal. The 2024 National Comparative Audit (NCA) of National Institute for Health and Care
Excellence (NICE) Quality Standard QS138 again highlights persistent deficiencies, particularly poor
documentation and limited evidence that patients are consistently informed about risks, benefits, or
alternatives before transfusion (NCABT, 2025). These findings reinforce the long‑standing concern that current practices fall short of what NICE QS138 expects.
Significant national updates aim to address these gaps.
The advisory committee on the Safety of Blood, Tissues and Organs (SaBTO) consent guidance,
updated in November 2025, strengthens standards for informed consent, shared decision-making, and clear documentation, replacing the 2020 guidance. These updates emphasise that consent must be a meaningful conversation, ensuring patients understand why a transfusion is recommended, the potential risks, and what alternatives may exist. A British Society for Haematology (BSH) position statement is also in preparation to provide further professional consensus and practical support.
Across the system, there is an urgent need to embed shared decision-making as routine practice.
National evidence shows that the provision of information and documented consent has not improved in recent years, underscoring the necessity for cultural change, better training, and more consistent communication with patients and families (Murphy, et al., 2025).
Digital innovation presents a powerful opportunity to transform how consent is supported. The My
Transfusion app, co‑developed by SHOT with patients and clinicians, provides clear, nationally aligned information on transfusion risks, benefits, options, and safety checks. It is the UK’s first dedicated transfusion information app, designed to empower patients and their families by enabling them to explore information at their own pace and prepare for consent discussions. It has been praised as an accessible, patient‑centred solution that enhances understanding and supports genuinely shared decision-making (see ‘Recommended resources’). The key challenge ahead is promoting widespread adoption of the app and addressing implementation gaps. Ensuring frontline clinicians are aware of and actively using My Transfusion within the consent process will be essential to realising its potential impact.
To support services further, a driver diagram has also been produced by SHOT to help teams identify
local barriers and plan targeted improvement actions related to consent and shared decision-making
(see ‘Recommended resources’). Strengthening communication, consistently documenting discussions, enhancing shared decision-making, and integrating digital tools like My Transfusion into routine practice are critical steps towards improving patient safety and experience across the transfusion pathway.
Laboratory safety
The IBI report emphasises the essential role of laboratory safety in enabling safe transfusion practice.
Although fundamental to patient care, laboratory risk is often underestimated until incidents occur.
Transfusion‑related laboratory errors continue to be persistently high especially with avoidable incidents (see Chapter 18, Laboratory Errors), underlining the urgent need for improvement. These issues persist due to systemic pressures, including insufficient staffing, high workloads, inconsistent training, and weaknesses in leadership and safety culture. Both the UK Transfusion Laboratory Collaborative (UKTLC) survey, due to be repeated later this year, and the safety culture survey continue to highlight these concerns, reinforcing that safer, more supportive laboratory environments are critical.
A stable, well‑trained workforce is central to delivering safe transfusion services. Improving staff retention, strengthening engagement, and fostering better collaboration all contribute to a safer system. Structured communication, effective handover processes, and proactively addressing gaps are vital to ensuring that every blood component is tested, stored, and issued correctly.
Optimising laboratory safety must now be a priority. This requires vigilance, robust staff training,
appropriate staffing levels, and a commitment to continuous improvement to safeguard patients and
support the teams who deliver this essential service.
Digitisation
Safe and effective digitisation of transfusion services is now a national patient safety priority. Digitisation, traceability and robust information systems were identified as a key recommendation of the IBI, reflecting the central role of accurate records, transparency and system reliability in preventing harm and enabling learning (IBI, 2024). In parallel, NHS England’s recently published digital maturity assessments, highlighted in national commentary including Health Service Journal, demonstrate wide variation in digital capability across providers, reinforcing the need for targeted improvement rather than uniform assumptions of readiness (Sollof, 2024; NHSE, 2026).
Haemovigilance data continue to show that errors related to IT are increasing, with recurring and
well‑recognised themes reported to SHOT, including poor system design, interoperability issues,
configuration problems, workarounds and inadequate training. These issues remain evident in Chapter 19, Errors Related to Information Technology (IT), underlining that digitisation alone does not equate to safety if systems are poorly implemented or optimised. The SHOT UK Collaborative Reviewing and reforming IT Processes in Transfusion (SCRIPT) survey conducted earlier this year will provide valuable frontline insight into digital transfusion practice and will help inform prioritised improvement activities by identifying system strengths, gaps and user‑reported risks. The analysis is ongoing, and the results will be released later this year.
Recent Health Services Safety Investigation Body (HSSIB) thematic reviews of electronic patient
record (EPR) systems highlight similar and persistent safety themes across healthcare. These include
missed, delayed or incorrect care arising from systems that do not meet clinical needs, inadequate
governance, insufficient user involvement, and failures to apply human factors principles during design and implementation. These findings reinforce the urgent need to modernise and digitise transfusion pathways, while being explicit that digitisation must be practical, safe and needs‑led, rather than technology‑driven (HSSIB, 2025a; Wise, 2025).
As digital transformation accelerates, it is essential that clinical and laboratory IT systems used in
transfusion are standardised where possible, meet national safety standards, and are supported by
appropriate training and competence. Subject‑matter experts from clinical transfusion and laboratory services must be meaningfully involved throughout procurement, configuration, implementation and optimisation, and systems must be designed and deployed in line with human factors and ergonomics principles to minimise new risks. New and updated national clinical safety standards for health IT systems (including DCB0129 and DCB0160 and associated NHS England guidance) provide a critical framework to support the safe use of digital systems in transfusion and should underpin all local digitisation programmes (NHSE, 2023; NHSE, 2025a). A set of essential standards for safe transfusions for clinical IT systems has been developed and released.
Shaping a learning health system rooted in care and progress
Learning health systems matter because they create the conditions for care to improve from within, rather than relying on occasional external scrutiny. The Health Foundation describes learning health systems as those that systematically use data, evidence, and experience from routine care to drive continuous improvement, with priorities including data use, digital capability, learning culture, and implementation at scale (accessible at these links: https://reader.health.org.uk/learning-health-systems/what-are-learninghealth-systems-and-why-do-they-matter and https://www.health.org.uk/reports-and-analysis/reports/developing-learning-health-systems-in-the-uk-priorities-for-action).
In transfusion, this is particularly important because the same types of incidents continue to recur: wrong blood in tube events, patient identification failures, delayed recognition of harm, ineffective handover, and variation in practice. These are not simply technical errors; they reflect inadequate system design, organisational culture, and the degree to which learning is translated into action, and sustainable change.
The uncomfortable question is whether we are truly a learning system yet. Despite several inquiries,
reports, and repeated recommendations, there is a lack of sustained change. Too frequently, learning
stops at the point of publication: recommendations are accepted, but ownership is diffuse, implementation is inconsistent, and impact is rarely evaluated over time. In that sense, the problem is not the absence of lessons, but the absence of reliable mechanisms to convert lessons into durable reform.
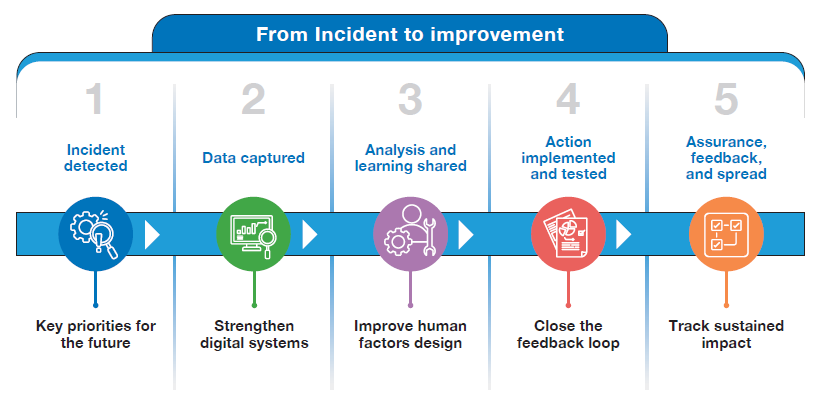
Transfusion safety can drive wider healthcare improvement by modelling how to close the loop from
incident to analysis, action, and assurance. This requires measurable change, human‑centred and digital solutions, and accountability for proven improvement- not just intent, so the healthcare system visibly learns, acts quickly, and sustains change.

Figure 4.3: From incident to improvement
Conclusion
The SHOT Transfusion Safety Standards provide a clear, structured and consistent framework for
embedding safe transfusion practices into everyday work, ensuring that safety becomes part
of organisational culture rather than an optional aspiration. By defining expectations, establishing
benchmarks, and supporting regulatory assurance, the standards create a foundation for meaningful,
measurable improvement. They offer a systematic method for addressing known risks and help
organisations focus their resources on the interventions that matter most for patient and staff safety.
However, the concerning signals highlighted in this year’s Annual SHOT Report leave no room for
complacency. They expose a hard truth: without urgent action, our current systems are not only
unsustainable; they are unsafe.
Almost two years after the release of the IBI report, progress on implementing its recommendations
has been far too slow. There remains no dedicated funding to support the scale of system change
required, despite the Inquiry’s clear and compelling mandate. To date, much of the progress across the transfusion pathway has happened only because of the commitment, professionalism, and resilience of individuals within the transfusion community, who continue to drive improvement without the structural support or resourcing they need. This reliance on goodwill is not a sustainable strategy, nor is it fair. Meaningful, national‑level change can only occur when clear funding is allocated, when implementation is prioritised, and when healthcare organisations are supported to redesign systems rather than simply absorb additional expectations. Without this, both patients and staff remain exposed to risks that are avoidable and unacceptable.
We must act now.
The warning lights are flashing red, signalling that delay and underinvestment are no longer tenable. To rebuild trust, restore safety, and honour the lessons of past failures, urgent decisive action is required across the health system.
Our collective call to action is clear and immediate:
- Protect and support staff by investing in wellbeing, safe staffing, protected training time, and psychologically safe working environments.
- Allocate dedicated funding to enable the full and timely implementation of the Infected Blood Inquiry recommendations.
- Prioritise the SHOT Transfusion Safety Standards within organisational and national safety agendas, ensuring they are embedded into daily practice, governance, and decision‑making.
- Strengthen systems, using technology, human factors principles, and robust processes to reduce
avoidable errors and variation. - Maintain safety for patients, donors, and staff as a non‑negotiable imperative, recognising it as the
core measure of quality and trust within the NHS.
The time for incremental change has passed. The system must now move decisively—from relying on
individual dedication to delivering coordinated, funded, and accountable action. Our responsibility is clear: to build safer systems, safeguard our workforce, and ensure that patients receive the safe, dependable transfusion care they deserve.
Recommended resources
SHOT Transfusion Safety Standards
SHOT patient information page
JPAC transfusion information for patients
UKTLC surveys
National Comparative Audit: 2024 Audit of NICE Quality Standard QS138
SHOT Essential Standards for Safe Transfusion in Clinical IT Systems
