Authors: Emma Milser and Alison Watt
Link to PDF chapterKey SHOT messages
Key findings
- New Human Factors Investigation Tool (HFIT) action effectiveness questions show good engagement and provide early insight into how learning from investigation findings is translated into action.
- Staff fatigue is an under-recognised patient safety risk.
Gaps identified
- Mismatches between workload and staff provision and issues related to written or verbal communication continue to be reported.
- Organisational pressures and fatigue-related risks are not always fully considered during event reviews.
- Actions implemented are often at the people-focused end of the hierarchy of effectiveness and do not consistently address the identified system factors contributing to errors.
Good practice
- SHOT reporters showed strong engagement with newly introduced HFIT questions on action effectiveness.
- Human factors frameworks are increasingly applied in adverse event reviews.
- There is improving recognition of system and organisational contributors rather than focusing solely on individual performance.
Next steps
- Where long-term system actions are difficult to achieve, such as new information technology (IT) developments, reporters, investigators, or leadership should frame the action as system-focused by placing these requirements on the organisation’s risk register.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
Human Factors and Ergonomics definition
Human factors and ergonomics is the scientific discipline concerned with the understanding of
interactions among humans and other elements of a system.
Introduction
Analysis of transfusion-related errors demonstrates how human factors influence safety across everyday work, from communication and decision-making to the conditions in which staff operate. Consideration is given to staff fatigue, recognising the associated safety risks to staff and the potential impact on patient safety. Case review and HFIT data highlight recurring themes including communication, local working conditions, organisational pressures, and staff fatigue. The introduction of new questions within the HFIT in 2025 now enables assessment of the actions taken following investigation, providing new insight into the nature and effectiveness of corrective and preventive actions (CAPA) implemented in response to events.
Analysis of HFIT
A total of 3358 error cases were included in 2025, representing an increase in the error cases reported
in 2024 (n=3322).
In January 2025, the HFIT was revised to include up to three new questions capturing key actions
taken following the investigation of a safety event. This enhancement enables reporters to reflect on the effectiveness of CAPA using the hierarchy of intervention effectiveness. The introduction of these action effectiveness questions has seen strong uptake among SHOT reporters, providing valuable insight into the actions undertaken. Data from these questions are analysed here for the first time, covering the initial 12 months following their introduction.
Analysis shows that the majority of reports included one or more improvement actions that had been
undertaken following local incident investigation, indicating active follow up. A single action was recorded in 1227/3358 (36.5%) reports, representing the most common response. Two actions were recorded in 957/3358 (28.5%) reports, and three actions were recorded in 666/3358 (19.8%), potentially demonstrating more comprehensive action being taken. This year marked the first inclusion of questions on interventions following local incident investigations. Response rates were high with 2681/3358 (79.8%) reports providing details of at least one completed intervention, indicating strong staff engagement. The insights obtained enhance understanding of post‑incident improvement actions, with particular relevance to the application of the hierarchy of interventions.
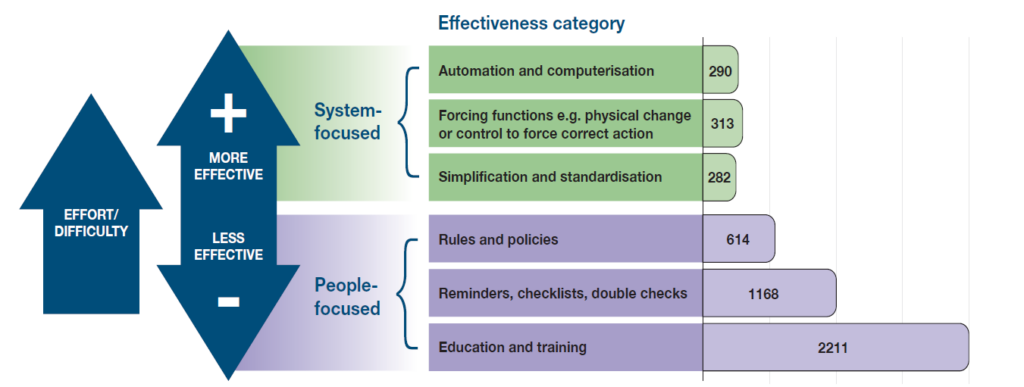
As illustrated in Figure 8.1, where action types are further disaggregated, education and training was the most frequently reported intervention across all categories, particularly among reports documenting a single action. Reminders, and rules and policies were also represented, while forcing functions, automation and simplification appeared less frequently. This distribution suggests a predominant reliance on single, education-based interventions, with comparatively fewer reports reflecting multi-layered or system-level approaches.
Figure 8.1: Number of improvement interventions by effectiveness category in 2025 (n=4878)
The SHOT HFIT, introduced in 2016, was designed to support a structured, systems-based approach.
Over the past decade, the HFIT has undergone multiple refinements to strengthen staff awareness of HFE concepts, improve investigative questioning, and support the identification of true causal and contributory factors. Throughout SHOT’s historical analysis of HFE, there has been evidence of an overemphasis on blaming individuals. Over the past decade, the HFIT appears to have supported a shift from attributing incidents to individual error towards recognising wider system interactions. Growing familiarity with HFE principles suggests improved confidence among investigators in identifying contributory factors, reinforcing a move away from a focus on individual error, which is less effective for safety improvement, towards system and organisational factors that enable more robust interventions.
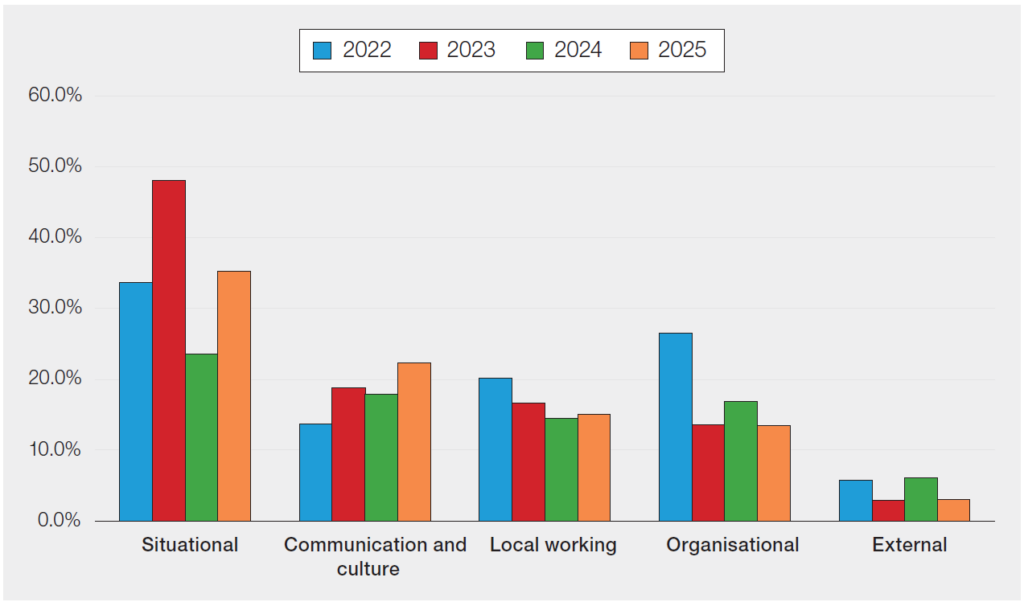
Figure 8.2 shows consideration across the breadth of factors for data between 2022-2025, with a marked increase of 751/3358 (22.4%) attributed to communication and culture factors. Within the organisational factors category, 585/3358 (17.4%) reported that organisational pressures played a role in the event, and 992/3358 (29.5%) indicated that there were gaps or issues with staff knowledge. For local working conditions around the time of the event, 1118/3358 (33.3%) stated that there was a mismatch between workload and staff provision. Where long-term system actions are difficult to achieve, such as new IT developments, reporters, investigators or leadership may frame the action as system-focused by placing their requirements on the organisation’s risk register.
Figure 8.2: A comparison of HFIT categories assigned by SHOT reporters in 2022-2025
The 2021 Annual SHOT Report recommendation that a ‘tried and tested human factors–based
framework’ be applied to investigations remains relevant (Narayan, et al., 2022). There is an encouraging continuing upward trend over the past five years, with more cases being investigated using a formal framework to consider human factors. For 2025, 2678/3358 (79.8%) cases specified that HFE principles or a framework/model were used to investigate incidents, and a further 228/3358 (6.8%) indicated they were planning to do so in the future.
Overall staff wellbeing
Staff wellbeing has been explicitly prioritised in the SHOT Transfusion Safety Standards, recognising its importance not only for individual resilience but also as a key organisational patient safety factor. Staff fatigue, in particular, has been highlighted due to its historically under-recognised impact. It remains a significant human factors issue that can compromise patient safety by impairing attention, decision-making, and situational awareness, and is influenced by workload, shift patterns, staffing levels, and organisational expectations (HSSIB, 2025).
The true prevalence of staff fatigue remains challenging to establish due to limitations in current reporting and monitoring mechanisms. Furthermore, fatigue may be influenced by underlying chronic illnesses among staff, which can both worsen symptoms and contribute to fatigue. Over a decade ago, a research clinic reported fatigue was a significant and debilitating symptom affecting up to 25% of the population (Hackett, et al., 2015). A recent investigation by the Health Services Safety Investigations Body (HSSIB, 2025) found that fatigue contributes both directly and indirectly to patient harm but is often viewed primarily as a wellbeing issue rather than a patient safety risk.
Addressing fatigue requires a systems-based response. This includes recognising fatigue within
governance processes, designing rotas that support rest and recovery, enabling staff to take breaks,
and fostering cultures where concerns about tiredness can be raised without stigma, even if due to
personal, family, or health issues. Human factors principles emphasise designing work systems so that safety does not depend solely on individual vigilance or resilience. This reinforces the importance of explicitly considering fatigue and organisational pressures within error analysis and learning reviews, ensuring that improvement actions address contributory system factors rather than focusing solely on individual performance. Leadership plays a central role in this, influencing whether fatigue is treated as an inevitable consequence of service pressure or as a manageable safety risk requiring proactive organisational action. The Medicines and Healthcare products Regulatory Agency (MHRA) endorses supporting staff openness on fatigue as a management responsibility. Consistent with this approach, fatigue will be incorporated as a standalone question within the HFIT at its next scheduled review.
Case 8.1: An avoidable transfusion in the context of system pressure and staff fatigue
A patient presented to the emergency department (ED) with abdominal pain, vomiting and diarrhoea, and suspected rectal bleeding at home, raising concern for a possible gastrointestinal bleed. Initial point-of-care testing (POCT) in ED, including arterial blood gas, showed a haemoglobin (Hb) of 64g/L and platelet count of 86×109/L. Coagulation testing also indicated deranged clotting parameters. On the basis of these results, which were consistent with blood loss and coagulopathy, the patient was transfused with two units of red cells and two units of fresh frozen plasma.
Following transfusion, the patient was transferred to a ward, where repeat laboratory testing
demonstrated a Hb of 155g/L and platelet count of 187×109/L, and improved coagulation results. These results were not clinically consistent with the components administered, nor with the patient’s high body mass index, and would not be expected following the transfusion support that the patient received. This discrepancy prompted immediate concern among clinicians regarding the validity of the initial POCT and coagulation results. On review, it appeared highly likely that the initial sample analysed in ED had been taken from the wrong patient, resulting in erroneous laboratory values being attributed to this patient.
At the time of the patient’s presentation, the ED was operating under sustained environmental and organisational pressure, including overcrowding, patients managed in corridors, high workload and frequent interruptions. The report highlighted that staff were working while fatigued as a result of ongoing operational strain, and there had been a recognised trend of sampling errors within the department associated with inconsistent adherence to safe patient identification and sampling procedures.
Under such conditions, adherence to safe sampling practices is more difficult to maintain due to increased cognitive load and exhaustion. The error in this case was therefore consistent with predictable human limitations within a pressured system, rather than individual staff failure.
The incident review was fed back to the ED Practice Development Team, and the primary action taken was staff education and training. While education may increase awareness, this response focused on individual behaviour and did not address wider contributory factors such as fatigue, workload, staffing levels or environmental constraints. The ongoing risks associated with organisational pressure and staff fatigue would be more appropriately recognised through inclusion on relevant risk registers and mitigated through system-level controls alongside training.
Learning points
- Staff fatigue and organisational pressure are recognised human factors risks that may compromise patient safety.
- Errors occurring in pressured environments may represent system vulnerabilities.
- Education alone has limited impact when organisational and fatigue-related risks are not addressed.
Conclusion
HFE provides a structured and evidence-based way of understanding safety beyond individual actions. By addressing system design, workload, leadership, and context, organisations can move from reactive responses to sustainable improvement. The themes outlined in this chapter reflect evolving thinking in transfusion safety and provide a foundation for the detailed data analysis presented elsewhere in the Annual SHOT Report.
A key addition to the analysis this year comes from the new questions asking reporters to record up
to three actions taken as a result of the event and categorise the effectiveness (Figure 8.1). While
consideration of wider system factors is increasingly evident, the interventions identified remain
predominantly focused on individual actions rather than addressing the underlying system gaps. This
represents missed opportunities for sustained and systemic improvement.
Patient safety could be improved by considering ways to mitigate issues related to staff fatigue. Dealing with fatigue is not simply a wellbeing issue, i.e. not only requiring people-focused actions but a system-wide change plan. These discussions are a reminder that a conclusion of ‘human error’ is an inappropriate outcome of an investigation. SHOT and the MHRA are aware that ‘human error’ is a category in the Blood Safety and Quality Regulations (Department of Health, 2005), and this is unlikely to change in the near future, but reporters are strongly encouraged to look beyond that as a final conclusion. Applying human factors principles in the analysis of transfusion error reports supports a deeper understanding of the underlying issues that need to be addressed to ensure safer systems are put in place. In addition, SHOT has introduced the use of the HFIT within the cell salvage category in 2026 to further enhance understanding; this will be reflected in the next Annual SHOT Report.
Recommended resources
SHOT Human Factors and Ergonomics (HFE) website page
Holistic approach to safety SHOT website page
SHOT Bite No.38b: Staff fatigue and transfusion safety – Practical solutions