Authors: Megan Rowley, Naim Rahimi and Jennifer Davies
Link to PDF chapter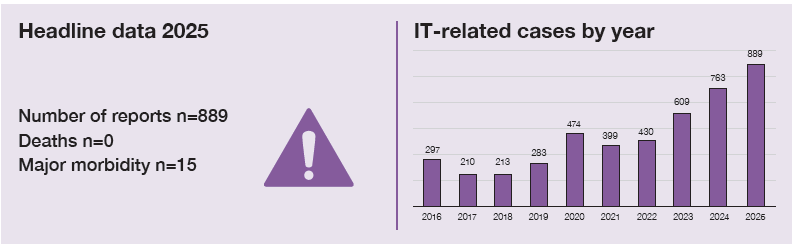
Key SHOT messages
Key findings
- The trend of increasing IT-related error reports continues with 16.6% more cases reported to SHOT in 2025 compared to the previous year.
- Errors relating to the use of flags, alerts and warnings accounts for 17% of reported incidents.
- The category where ‘IT could have prevented’ the error now comprises 28% of all cases included, reflecting the increased recognition by staff of the role of IT systems in supporting safer transfusion practice.
Gaps identified
- Poor interoperability between clinical and laboratory systems continues to contribute to avoidable errors.
- Usability issues identified in analysed errors include unclear, poorly timed, or misinterpreted alerts and warnings.
- Evidence of limited end-to-end testing of interoperable systems contributing to unintended consequences in practice.
- Periods of system downtime and IT go-live identified as high-risk, highlighting the need for robust validation, preparation and contingency planning.
- Suboptimal ergonomic design of software and equipment is contributing to human-system interface failure.
Good practice
- Increasing use of electronic blood management systems demonstrating progress towards integrated vein-to-vein IT systems, in line with recommendations from the Infected Blood Inquiry.
Next steps
- Using insights from the recent SHOT United Kingdom (UK) Collaborative Reviewing and reforming IT Processes in Transfusion (SCRIPT) IT survey, further improvement actions to be initiated to improve transfusion IT systems across the UK.
- Hospitals should undertake a gap analysis against the SHOT Essential Standards for Safe
Transfusion in Clinical IT Systems and update systems accordingly.
Glossary, acknowledgments and reference list
Please access these links for the Glossary for all abbreviations, Acknowledgments and References used.
SHOT category definition
IT-related incidents definition
This chapter includes transfusion adverse events that relate to laboratory information management systems as well as other information technology systems and related equipment used in the delivery of hospital transfusion services.
Cases selected include events where IT systems may have caused or contributed to the errors
reported and where IT systems have been used incorrectly. Where the corrective and preventive action suggested by hospitals in response to errors included IT solutions, these have been included.
Introduction
IT systems play an increasingly central role in the delivery of safe transfusion practice, supporting
decision-making processes, communication and traceability across the vein-to-vein pathway. Reflecting this growing reliance on digital systems, the total number of IT-related errors reported to SHOT has increased in this reporting year, from 763 in 2024 to 889 in 2025. This is likely to represent, at least in part, increasing system use, wider digital coverage across transfusion pathways, and improved recognition and reporting of IT-related contributory factors to transfusion safety incidents. Importantly, over a quarter of these reports were cases where IT was identified as a corrective and preventive action (CAPA), rather than a primary cause for error. This reflects increasing recognition of the potential for IT systems to support safer transfusion practice when appropriately designed, configured, and used.
The SHOT Transfusion Safety Standard 2 relating to transfusion IT and equipment, sets out key
expectations reflecting the previous SHOT recommendations for transfusion IT systems. This includes
system functionality, interoperability, reduction of manual data transfer, appropriate alerts and staff
training. These principles provide an important framework for understanding IT-related transfusion errors, particularly where systems are relied upon to support complex clinical and laboratory workflows. Many of the errors described in this chapter reflect challenges in consistently meeting these standards in practice.
Deaths related to transfusion n=0
There were no deaths attributable to IT errors.
Major morbidity n=15
There were 15 cases where IT errors may have contributed to major morbidity. A few cases have been
discussed in detail in relevant chapters (see Cases 9.1, 10.1, 10.9, 18.2 and 19.2).
Overview of cases
The primary reporting category of the 889 cases included in this chapter is shown in Table 19.1. Of these, 776 were related to the transfusion of blood components, 105 to anti-D immunoglobulin (Ig) and 8 to prothrombin complex concentrate (PCC). Cases were identified if reporters indicated on the questionnaire that IT was implicated in the error. Analysis of the submitted reports helped identify additional cases where IT was involved. The reason for inclusion is summarised in Figure 19.1. There was a 16.5% increase in IT-related reports (n=889 in 2025 from n=763 in 2024), with the largest increases being in incorrect blood component transfused-specific requirements not met (IBCT-SRNM), IBCT-wrong component transfused (IBCT-WCT) and right blood right patient (RBRP) categories. A reduction in anti-D Ig administration errors was noted and there was little change in the avoidable, delayed, under or overtransfusion and handling and storage errors (HSE) categories. The errors attributed to the clinical area accounted for 548/889 (61.6%) of the total IT-related errors. The other notable change was the cases included where IT could have prevented the error, which accounted for 245/889 (27.6%) of reports (see Figure 19.1).
Table 19.1: Primary reporting categories containing errors related to IT in 2025 (n=889)
| Primary reporting category for IT cases | Laboratory errors | Clinical errors | Number of IT cases 2025 | Number of IT cases 2024 |
|---|---|---|---|---|
| IBCT-SRNM | 125 | 92 | 217 | 165 |
| RBRP | 52 | 155 | 207 | 138 |
| HSE | 59 | 99 | 158 | 143 |
| Anti-D Ig | 29 | 76 | 105 | 140 |
| IBCT-WCT | 47 | 37 | 84 | 65 |
| Delayed transfusion | 19 | 55 | 74 | 65 |
| Avoidable transfusion | 8 | 24 | 32 | 33 |
| PCC | 2 | 6 | 8 | 11 |
| Under or overtransfusion | – | 4 | 4 | 3 |
| Total | 341 | 548 | 889 | 763 |
Figure 19.1: Distribution of cases across type of IT issues (n=889)
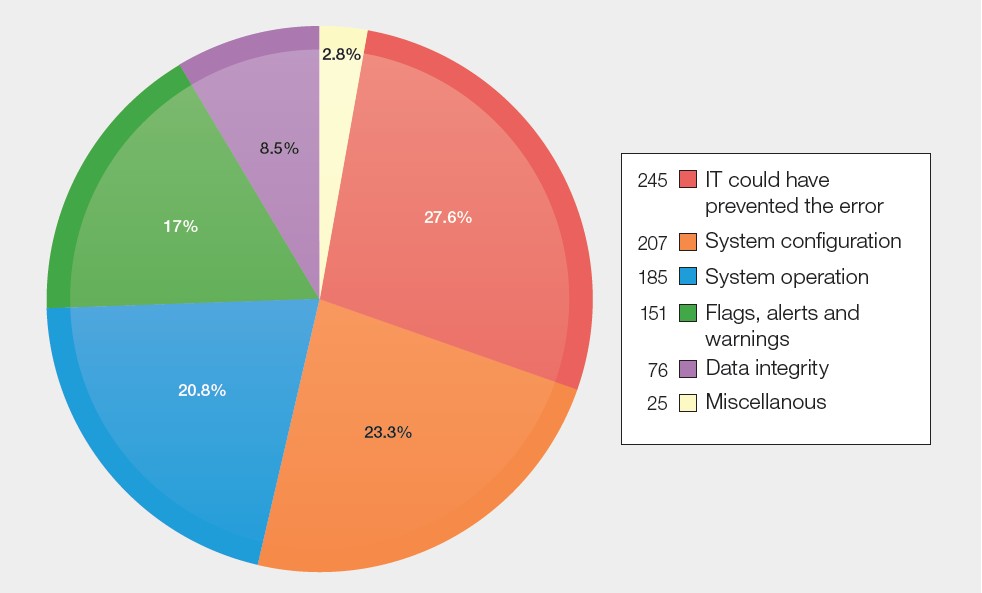
Flags, alerts and warnings n=151
Flags, alerts and warnings are used by IT systems to guide and advise operators at all stages of the
transfusion pathway and greatly enhance patient safety in both clinical and laboratory settings. There
were 55 cases where a warning flag was in place but was not heeded, 33 cases where a flag was not
updated in a timely or accurate manner or was disabled in error and 63 cases where flags, or logic
rules, were available but not used.
Case 19.1: Alert fatigue results in delayed transfusion
A patient requiring a second unit of red cells for a suspected upper gastrointestinal bleed experienced a delay in transfusion due to poor venous access and failures in electronic task management in an out-of-hours setting. Repeated electronic requests for venous access were sent to the hospital-at night team but were deleted, having been misinterpreted as historic or duplicate tasks based on the fact that the patient had been cannulated earlier, but this had stopped working after the first transfusion. No clarification was sought with the ward and reduced overnight staffing with competing clinical commitments further contributed to delay. The second unit was eventually administered once venous access was obtained.
Learning point
- Repeated electronic alerts in a busy, out-of-hours setting, combined with competing clinical priorities, can lead to assumptions being made and safety-critical messages being dismissed without verification.
Data integrity n=76
Data on IT systems must be both accessible and accurate. There were 18 cases where the wrong
computer record was accessed, 20 cases where incorrect information was entered or accessed manually, 28 cases where computer records were not linked, merged or reconciled leading to missing information and a further 10 cases where the historical record was available but not consulted.
Software configuration n=207
Although IT systems can enhance patient safety, they must be up-to-date, compliant with national
guidelines and configured correctly (MHRA, 2010; Milkins, et al., 2013; NHSE, 2025b). There were 123
cases where the IT system lacked the functionality or algorithms to support safe transfusion practice
and a further 27 cases where IT systems were not configured correctly. Interoperability between systems reduces errors associated with manual data transfer and repetitive and duplicative data entry. There were 57 cases where an error occurred because of lack of interoperability or interfacing.
Case 19.2: Delay in issue of emergency blood following new laboratory information management system (LIMS) go-live
A patient undergoing emergency bowel surgery developed significant intraoperative bleeding
requiring activation of the major haemorrhage protocol (MHP). Laboratory staff experienced repeated failures when attempting to electronically issue compatible red cell units due to an error message that appeared when scanning a group & screen sample. Two valid samples were present in the laboratory; however, the more recent sample had invalidated the older one, and the system did not clearly guide users to the appropriate sample, resulting in repeated scanning attempts against the incorrect barcode. This situation had not been anticipated or tested during pre-implementation validation, and this was the first MHP activation since the LIMS go-live.
Learning point
- Limitations in system configuration can result in unintended consequences which become apparent following IT go-live. Systems must be in place to support timely escalation and prompt responses to address these post go-live.
System operation n=185
Staff using IT systems need to be trained and competent to use the system and there were 144 cases
where systems were not used correctly. When clinical and laboratory practice is dependent on equipment and IT systems, there must be robust business continuity plans and downtime procedures to enable transfusion to safely continue when these are not available. There were 41 cases where planned, or unplanned, system downtime led to errors. These include malicious cyber-attacks as well as technical failures and planned downtime to upgrade systems.
Case 19.3: Lack of familiarity with contingency plans during cyber-attack led to delay
During a cyber-attack incident, the LIMS was unavailable, and an interim process was introduced requiring prior authorisation of blood provision for surgical patients from the clinical haematology team. A patient undergoing coronary artery bypass graft surgery, who was borderline anaemic and likely to require perioperative transfusion, proceeded to theatre without compatible red cells being requested, authorised or prepared via the interim manual process. When the clinical team contacted the transfusion laboratory intraoperatively, they were informed that no blood had been approved, necessitating an urgent escalation to the on-call haematologist, resulting in an avoidable delay in blood provision.
Learning point
- In IT downtimes and cyber-attack-related IT outages, clear contingency processes should be in place which all relevant stakeholders should be familiar with.
IT could have prevented the error n=245
This category has greatly increased in recent years with 245 cases indicating that errors could have been prevented were IT systems in place and used appropriately to support patient safety. Whilst many of these were identified as corrective and preventive actions, the time and resources required to make a change to an existing IT system or procure and implement a new system are often cited by reporters as barriers to change.
Near miss (NM) events related to information technology n=597
Table 19.2: Near miss cases containing errors related to IT in 2025 (n=597)
| Laboratory | Clinical | NM cases 2025 | NM cases 2024 | |
|---|---|---|---|---|
| NM ‘other’ | 127 | 126 | 253 | 181 |
| NM-wrong blood in tube (WBIT) | – | 344 | 344 | 220 |
| Total | 127 | 470 | 597 | 401 |
Figure 19.2: Proportion of near miss cases identified as belonging to IT error categories in
2025 (n=597)
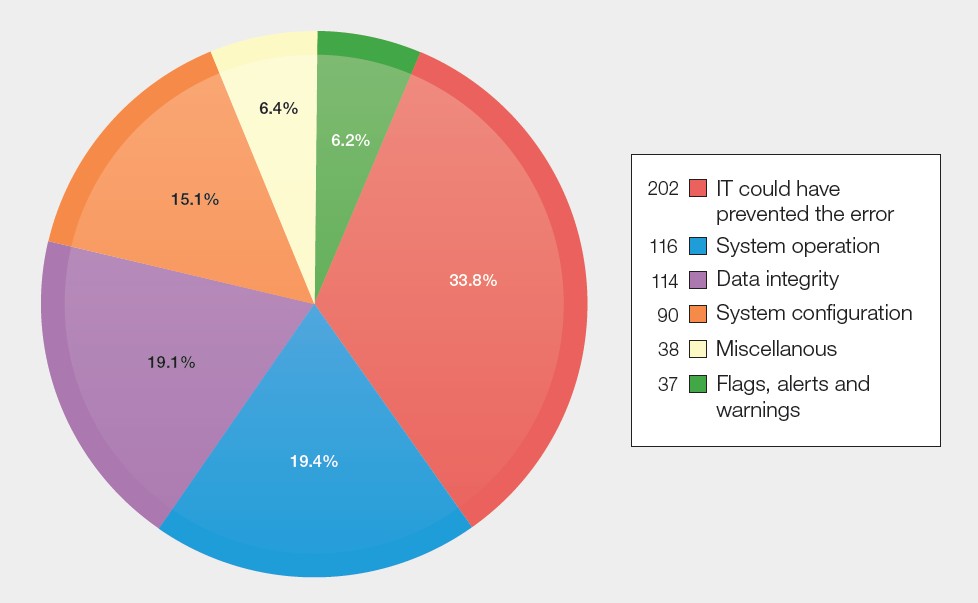
Near miss ‘other’ IT events n=253
The reporting categories for the near misses were as follows: NM IBCT-WCT 89, NM RBRP 54, NM IBCT-SRNM 47, NM HSE 42, NM anti-D Ig 14 and NM ADU 7. Just over half of the errors were attributable to
the laboratory, 127/253 (50.2%) and 74/253 (29.2%) were included because IT could have prevented the error, had it been in place. Three cases were noted where IT detected the error (2) or prevented the error (1). Lack of interfacing and/or interoperability contributed to 23 near misses and in 31 cases, the IT system in use did not have algorithms to support safe practice or lacked the necessary functionality. In 41 cases, the system was not used correctly. In 9 cases, there was failure of the IT system or other equipment.
Near miss wrong blood in tube (WBIT) n=344
These were all clinical errors, by definition, and 125/344 (36.3%) were included because IT could have
prevented the error, had it been in place or IT systems were introduced but not being used. The most
common reason leading to WBIT that involved IT was selecting the wrong patient details from the IT
system, 88/344 (25.6%). Various issues related to IT system configuration were noted in 33 cases. Of
these, in 24, the system was configured incorrectly, 5 where the functionality or algorithms to support safe practice were not in place and 4 cases attributed to lack of interfacing or interoperability. There were 45 cases where the system was used incorrectly. System or equipment failures were implicated in 21 cases, of which 4 related to IT downtime and a further 2 cases related to a cyber security incident.
SHOT UK Collaborative Reviewing and reforming IT Processes in Transfusion (SCRIPT)
SCRIPT is a group of transfusion professionals representing the 4 UK nations bringing their experience and expertise in the use of IT to improve transfusion safety through shared learning and developing best practice resources. Many of the SCRIPT initiatives were identified following the 2020 hospital survey, and this has been repeated at the end of 2025. The results reflect current status with respect to implementing and improving clinical and laboratory IT systems across the UK. Following the Infected Blood Inquiry recommendation 7f(iii) ‘that funding for the provision of enhanced electronic clinical systems in relation to blood transfusion be regarded as a priority across the UK’ (Vickers, et al., 2025), a resource has been developed to describe the functionality of clinical IT systems to support patient safety. This has been led by colleagues from the National Transfusion Practitioners Network. In collaboration with SCRIPT and stakeholders across the UK, the ‘Essential standards for safe transfusion in clinical IT systems’ has been released. This document can be used to support procurement and implementation of new systems as well as reviewing existing systems to see if they can be improved. To further support and inform transfusion professionals a 3-part e-learning module IT in transfusion on this subject is in production and will be launched shortly.
Conclusion
IT-related transfusion errors rarely arise from isolated technical failure; rather, they reflect breakdowns at the human-system interface, including usability challenges, alert fatigue, workarounds and increased cognitive load during periods of high workload or system instability. This chapter therefore considers not only the functionality of IT systems but also how staff interact with them in real clinical or laboratory environments, emphasising the importance of user-centred, end-to-end design that reflects real-life clinical and laboratory workflows across the transfusion pathway.
Cyber security threats and both planned and unplanned system downtime continue to present significant challenges to transfusion services. Several cases in this reporting year highlighted the impact of system outages, including those resulting from cyber-attacks, on the timeliness and safety of transfusion. These events underscore the importance of robust, well-rehearsed contingency and business continuity plans that enable safe transfusion practice when IT systems are unavailable.
Interoperability between clinical and laboratory systems remains a recurring theme. Lack of effective data exchange, including between electronic patient records, LIMS, electronic blood management systems, and specialty systems, continues to contribute to errors, delays, and duplication of work. The phased rollout of specialty systems, in neonatal and maternity services without adequate integration with the existing systems, has introduced additional complexity where transfusion-relevant information must be manually transcribed between systems as discussed in Chapter 9, Adverse Events Related to Anti-D Immunoglobulin (Ig). This reliance on manual data transfer increases the risk of omission, transcription error, and loss of situational awareness, particularly in high-acuity environments.
Recommended resources
SCRIPT resources including aide memoire for IT downtime and presentation on unexpected
IT downtime
Information Technology (IT) Errors Cumulative Data page
SHOT Essential Standards for Safe Transfusion in Clinical IT Systems
